It's funny how oblivious Americans are to the dangers of driving. This despite generally knowing people who have been badly injured or killed in vehicular accidents.
Car exhaust is also a big deal. Air pollution kills.
Instead of talking about the very concretely understood dangers of car culture, people want to spout total nonsense about sugar or freak out about a little second hand smoke.
Another big difference in the American way of life is that, in most cities, we've managed to engineer a wholly car-dependent transportation system, such that the average American walks half as much people in other countries:
http://well.blogs.nytimes.com/2010/10/19/the-pedometer-test-...
All that driving also puts the average American at huge risk for dying young in a car crash.
One of my more memorable events back when I lived in a suburban cul-de-sac as a teenager was walking home from school and finding a neighbor's 4-year-old stumbling into the street, blind with tears. Her mom hadn't noticed that she wasn't in the car when she drove out.
I know it is hard to control for culture, but seeing as how mormon men are still American but have a 10 year gap in life expectancy over other American men [1], any analysis on the effects of health care across nations should at least try to control for cultural differences. That singular cultural difference is twice the magnitude of the difference between the OECD and the US. And when you realize that culture could be a far stronger predictor than health care quality/availability, you start wondering how much of that gap is due to us being fatasses.
> I know it is hard to control for culture, but seeing as how mormon men are still American but have a 10 year gap in life expectancy over other American men
The study [1] did not find that Mormon men have a 10 year advantage of other American men, it found that the "optimum" subgroup of white Mormon men ("optimum" defined as never smoked, married, 12+ years education, and at least weekly church attendance) had a 9.8 year life expectancy advantage over white males in general in the US -- and that similar figures were seen for the same "optimum" characteristics among all religions.
The typical american lifestyle seems designed to kill you: drink a lot, work all the time, take drugs (legal or otherwise) to medicate or recreate yourself into submission, refuse to use your 10 days a year off so you continue to look like a "team player."
The mormon lifestyle is: no drinking, everything is based around family/community, and travel the world to convert others. Plus, something about a musical.
Fun fact: A few tech companies refuse to recruit at BYU because mormons can't work all weekend.
If you look at the original study, the biggest single-factor difference (and its not Mormon men that have the 10 years advantage, but Mormon men that have never smoked, have 12+ years of education, are married, and attend church at least once a week) is "never smoked", and the next strongest is "attend church at least once a week" (though whether that's causal or covariant is at least debatable).
And unique features of Mormon practice presumably aren't involved, since the study found the same improvement for members of other religions with the same identified "optimum" features.
No smoking, no drinking alcohol, coffee or tea (I think it may be caffeine). They also tend to have a stronger focus on homemade food (rather than pre-cooked/boxed/canned) and habits/hobbies that aren't dangerous.
In other words, all of the fun, yummy, or convenient, but terrible for you things that tend to be in our lives, they're not allowed to do.
A few others that come to mind not related to food/drinks:
* Absolutely no work on Sundays (not even checking work email)
* A strong social safety net. Mormons are expected to tithe (pay 10% of their income to the church), and this is used in part to provide for members in need. Extensive volunteering is also expected, and used for some of the same purposes (e.g. caring for elderly or disabled).
Mormons are expected to have lower or no consumption of alcohol, tobacco, and illegal drugs (and it's fairly more difficult to obtain at least the former two in Utah). Though, I can't find any actual study data showing they do in fact have lower consumption of those, it would be interesting to see if anyone has some data showing they are in fact lower.
It's once a month, and is a two-meal fast of both food and drink. Another concrete cultural practice that could make a difference is that Mormons abstain from alcohol, coffee, tea, and tobacco.
Life expectancy per cup of coffee consumed each days peaks at 2 cups a day. Which doesn't actually prove anything, but is at least suggestive. There are a whole bunch of health effects related to coffee, but in general you can get all the benefits with moderate consumption, but the negatives are in proportion to dose.
> Well, I wouldn't say drinking coffee or tea is a health benefit. Especially coffee.
OK. But that doesn't tell me much. :)
I brought this up because it has been conventional wisdom up until recently that you'd do better health-wise without coffee, while recently the topic has seemed to become more nuanced. Wikipedia lists both health risks and health benefits. It's not clear, to me, that it is straightforward to balance all the purported benefits and downsides and land on one or another conclusion.
As for tea, I have never seen that that is something that is unhealthy (assuming no extra ingredients like sugar). Conventional wisdom says that green tea is in fact very healthy. I haven't read much about the effects of black tea.
Personally I drink both coffee and tea without adding anything to them.
The big ones have already been mentioned, but there's also daily prayer (you could call it meditation) and strong family ties. Also, a ton of volunteer work.
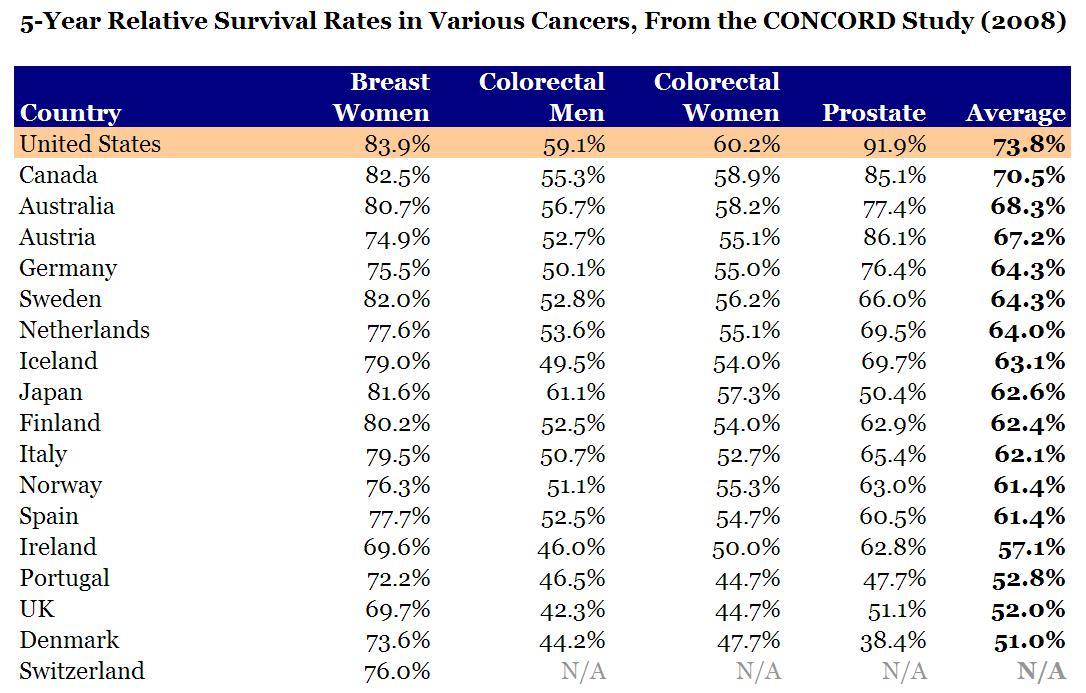
5-year survival rate is a poor statistic for comparing cancers across regions. It's highly correlated with how early the cancer was detected -- treatment effectiveness is just noise in comparison.
“It has been claimed (Ohsfeldt and Schneider, 2006) that adjusting for the higher death rate from accident or injury in the United States over 1980-99 than the OECD average would increase US life expectancy at birth from 18th out of 29 OECD countries to the highest. In fact, what the panel regression estimated by these authors shows is that predicted life expectancy at birth based on US GDP per capita and OECD average death rates from these causes is the highest in the OECD. The adjustment for the gap in injury death rates between the United States and the OECD average alone only increases life expectancy at birth marginally, from 19th among 29 countries on average over 1980-1999 to 17th. Hence, the high ranking of adjusted life expectancy at birth mainly reflects high US GDP per capita, not the effects of unusually high death rates from accident of injury. For information, the most recent data (which were used to make these calculations) on average standardised death rates per 100 000 population from accident or injury over 1980-1999 for land transport, uicides, homicides, and falls, respectively are 17.4, 11.4, 9.2, and 4.6 for the United States and 15.5, 13.3, 3.0, and 10.4 for the OECD average (OECD Health Data, 2008). Life expectancy at birth on average over 1980-1999 was 75.3 years for both the United States and the OECD average (29 countries) (OECD Health Data, 2008).”
Further Ohsfeldt and Schneider has never been formally published or peer reviewed.
This is untrue. Ohsfeldt and Schneider did not 'remove fatal injuries from life expectancy data', they used a regression analysis to adjust life expectancy values to equalise the number of fatal injuries. They have not actually dug deep to actually investigate whether fatal injuries does explain low life expectancies, only observed that there is a correlation.
This methodology is questionable, to say the least, and can potentially produce perverse results, and to my knowledge, they have not shown their working to show that they have not fallen into the many many pitfalls this method can generate.
The U.S. has greater income and healthcare inequality, and has a larger population of poor people living without access to reasonable medical care. The major impact of this on life-expectancy shows up in infant mortality rates, which is 6.14 per 1,000 versus 4 per 1,000 OECD average: http://www.nbcnews.com/health/us-infant-mortality-rate-drops....
The graphs in the article showslife expectancy at birth, which is a number dominated by infant mortality rate. For life expectancy at age 65, the US is slightly above the OECD average. Comparable to Germany or Norway. See Page 19 of this PDF: http://www.oecd-ilibrary.org/docserver/download/8109111ec004....
There's lot's of elements to the problem. For example, the infant morality rate for black Americans is double the rate for white Americans, and triple the OECD average: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6205a6.htm.
...and has a larger population of poor people living without access to reasonable medical care.
This is unlikely to affect the stats. Giving poor people access to health care does not improve physical health in any measurable way. It does make them feel better, however.
You can't possibly extrapolate from 5 years of data to impact on life expectancy.
Increased access to prenatal care has a very clear correlation with reducing early births (and that Oregon study focused narrowly on improvements in blood pressure, cholesterol or glycated hemoglobin. Reducing infant mortality isn't in there.).
Edit: Also, how much impact do you think earlier diabetes intervention will have in a 2 year period? I can at least conceive of earlier intervention having some impact after 5 or 10 years.
It certainly does make a difference for infant mortality, which is alleviated with proper pre-natal and post-natal care: http://www-personal.umich.edu/~baileymj/Bailey_Goodman-Bacon... ("Improved access to medical care resulting from the desegregation of hospitals and the initiation and expansion of Medicaid significantly reduced
infant mortality (Almond, Chay and Greenstone forthcoming; Goodman-Bacon 2013; Currie and Gruber 1996b). During the 1980s, acute neonatal care (neonatal intensive care units) helped less healthy infants survive. Improvements in access to medical care also reduced the mortality of older children, especially mortality due to common childhood diseases such as pneumonia and meningitis (11 percent of all childhood deaths). Medicaid coverage played an important role for poor children as it increased care for conditions easily treatable with antibiotics (Goodman-
Bacon 2013, Currie and Gruber 1996a).").
Of the various public health concerns, infant mortality is one of those that are most directly addressable with medical care directed at the poor. Improved access to health services won't get a poor person to change his diet, but can be very effective in catching potential complications from pregnancy, treating infections in neonates, etc.
Also, the study you linked-to doesn't support the claim you're making ("Giving poor people access to health care does not improve physical health in any measurable way."). The study looked at just three physical health outcomes, after two years: blood pressure, cholesterol, and glycated hemoglobin (a measure related to blood sugar level control). These are lifestyle-related measures unlikely to be affected in merely two years.
Moreover, the study is inappropriately designed to test the conclusion you assert. First, it is based on giving a random sampling of people access to Medicaid ("In 2008, the state of Oregon drew names by lottery for its Medicaid program for low-income, uninsured adults."). But to address lifestyle diseases, you need to build a culture of intervention over a long period of time. You can't do this in just a few years targeting a few members of the community. Second, the study doesn't measure the impact of "access to health care" but rather access to Medicaid. The non-control group still received healthcare services, they just did so through the emergency room and by doctors' visits that went unpaid ("Medicaid decreased the probability of having an unpaid medical bill sent to a collection agency by 25 percent.").
While I'm sure the lack of medical access and quality of are major contributors, I think this OECD document on obesity and overweight rates are telling as well:
The sugar- and grain-rich diet that has been aggressively promoted by the USDA for decades is responsible for a large part of this. The "low fat" mantra resulted in a lot of "fat free" but sugar-laden and/or grain based foods being the primary component of many diets, resulting in epidemic obesity and diabetes.
The USDA marketed equally to everyone, yet we see a wide gap in growth in life expectancy shows wide disparities between the poor and wealthy[1]. The growth of life expectancy of those with money has kept up with the OECD growth, while the life expectancy of the poor has largely stagnated.
>The "low fat" mantra resulted in a lot of "fat free" but sugar-laden and/or grain based foods being the primary component of many diets, resulting in epidemic obesity and diabetes.
This is because people can't read more than one thing, it's not a conspiracy on the part of the government.
Messages from the US government are correct, Americans in general consume too much fatty foods. That people can't look at what they're eating, see it contains 900% of their daily sugar intake and instead stop thinking at that bright 'LOW FAT' sticker on the front is not the governments fault.
And god damn, grains are a portion of the diet, they're not pushing a high grain diet. The food pyramid is 'all things in moderation' in an infographic form.
>Messages from the US government are correct, Americans in general consume too much fatty foods.
What are you basing this on? I've seen no controlled studies supporting the idea that saturated fats are harmful.
Anecdotally, I switched to a diet high in saturated fats and without grains or sugars, and my cholesterol numbers went from good to absolutely optimal, with high HDL and very low triglycerides. Friends on the same diet report similar results.
"For specific fatty acids the following is proposed: saturated fatty acid (SFA) and trans fatty acid intake should be as low as possible"
"There is a positive, dose-dependent relationship between the intake of a mixture of saturated fatty acids and blood low density lipoprotein (LDL) cholesterol concentrations, when compared to carbohydrates. There is also evidence from dietary intervention studies that decreasing the intakes of products rich in saturated fatty acids by replacement with products rich in n-6 polyunsaturated fatty acids (without changing total fat intake) decreased the number of cardiovascular events. As the relationship between saturated fatty acids intake and the increase in LDL cholesterol concentrations is continuous, no threshold of saturated fatty acids intake can be defined below which there is no adverse effect. Thus, also no Tolerable Upper Intake Level can be set."
No, no study concludes they need to be cut out (they don't), but to say there are no studies suggesting there are higher risks with higher fat intakes is not correct.
And just for your high fat diet and everything is cool:
Hooper, 2001 "There is a small but potentially important reduction in cardiovascular risk with reduction or modification of dietary fat intake, seen particularly in trials of longer duration."
One of the studies they reference:
"In March the American Journal of Clinical Nutrition published a meta-analysis—which combines data from several studies—that compared the reported daily food intake of nearly 350,000 people against their risk of developing cardiovascular disease over a period of five to 23 years. The analysis, overseen by Ronald M. Krauss, director of atherosclerosis research at the Children’s Hospital Oakland Research Institute, found no association between the amount of saturated fat consumed and the risk of heart disease."
Sugar is not bad for you. Fruit juices and sucrose in the context of adequate nutrition is good for you. Getting a fraction of your calories from sugar is a good idea.
I doubt grains are that big a deal for most people.
Unsaturated fats are the only thing in the diet that is clearly bad and people still eat loads.
Unsaturated fat (excluding trans fat) is good for you...this is one of the few things in nutrition that's entirely uncontroversial. I'm pretty sure you're thinking of saturated fat, but you're wrong about that too, since it's not "clearly bad". The fact that no one on either side of the theories around saturated fat seems capable of accepting is that the science is not yet firmly conclusive in either direction.
C.f.
http://www.scientificamerican.com/article.cfm?id=carbs-again...
"In March the American Journal of Clinical Nutrition published a meta-analysis—which combines data from several studies—that compared the reported daily food intake of nearly 350,000 people against their risk of developing cardiovascular disease over a period of five to 23 years. The analysis, overseen by Ronald M. Krauss, director of atherosclerosis research at the Children’s Hospital Oakland Research Institute, found no association between the amount of saturated fat consumed and the risk of heart disease."
I definitely mean that unsaturated fats are to be avoided. Saturated fats are quite safe, however large single sitting intakes are a bad idea because of increased endotoxin absorption. Monounsaturated fats are probably fine, but other unsaturated fats accumulate in tissues over time and cause disease. DHA is implicated in alzheimers. PUFAs, including omega-3, are tied to cancer and metabolic disorders. Even the so-called essential fatty acids are understood to interfere with the endocrine system over time.
Coconut oil and dairy fat are safe. Other fats should really be minimized. To the extent that any fatty acids are "essential" you'll easily get them incidentally from foods. All vegetable oils are bad for you and fish oils are bad for you.
Ah ok wow, my mistake. It's so common to hear people confidently (and wrongly) saying that saturated fats are DEFINITIVELY SCIENTIFICALLY PROVEN to be bad for you that I just assumed that you mistyped.
That being said, from what I can tell, unsaturated fats are a far cry from your claim of "clearly bad", and even farther from "the only thing in a diet that's clearly bad". From a quick Google search, it appears that there's preliminary evidence that high amounts of PUFAs increase the rate of metastasis in rats with cancer, and preliminary evidence that high amounts of PUFAs decreases the "all-cause mortality" rate and rate of cancer events in humans with cancer. With such a low bar for "clearly bad", one could dig up a thousand and one studies about refined carbs (let alone sugar) that make it infinitely more "clearly bad".
*I mean that in the sense of reading up on things from reliable sources (studies etc), not that I'm a researcher
The Amish present another interesting divergence from the general populace's life expectancy:
"[T]he Amish have had a 72-year life expectancy not only for the past few decades, as have most Americans, but for the last 300 years—since they settled in the United States in the 1700s, when most people living in America were dying in their 40s."
Was there really a time when most Americans were dying in their 40s (as opposed to 40 being the life expectancy from birth, which is a wildly different thing)?
I had no idea the two were different, so thanks for making that distinction. For anyone else's sake, I'll share what I learned:
Life expectancy from birth weights times of poor medicine and prenatal care towards the low end of the life expectancy scale because of much higher infant mortality rates, whereas in modern times life expectancy from birth would be weighted the opposite.
So basically, if you filter out infant mortality and other "first years of life" deaths, you get a more accurate picture of how long someone could actually expect to live if they make it past the initial thresholds to human existence.
Yeah, the problem is basically that historically you're most likely to die either very young or fairly old, but averaging out the ages at which people die creates the opposite impression — that you're likely to die sometime in your late 30s to early 40s, which was never actually the case.
Yeah, something weird is going on there. 72 years at birth for the Amish sounds absolutely crazy too. Maybe the Amish one is life expectancy at 5 or 20 and the other at birth.
It's possible that they simply have much lower rates of infant mortality. The linked discussion is from pay-walled researchers, so hard to see where they discuss their methodology.
Low incidence of alcohol use, strong communities with a tradition of midwifery, narrow genetic pool (which would tend to exaggerate any gene pool effects) are all things that could contribute to lower rates of infant mortality.
I wonder if the non-US OECD life expectancy might -- for some decades prior to 1990 or so -- have been excessively depressed by a couple of years. There are two major reasons I can think of for this. The first is that for at least the first half of the 20th century the U.S. population on average was probably substantially wealthier than European counterparts (European countries make up a substantial part of the OECD). The second is that the civilian population of much of Europe suffered much more during World War II. This might have resulted in lingering effects on life expectancy that gradually disappeared over the ensuing decades.
I think that it might explain part of the divergence. There are a couple of obvious reasons that the U.S. might trail the OECD -- the greater number of deaths due to higher car accident rates and a higher murder rate, as well as a well known disparity in the life expectancies of Americans of primarily European descent and those of people of primarily African descent.
I'm still trying to figure out how to say this. I'm wondering if the "natural" life expectancy in the U.S. has always trailed the "natural" life expectancy of the rest of the OECD (judged collectively, anyway) but because of some systemic effects in Europe this natural disparity was offset for some decades. The effect might have been something that gradually faded, exposing the natural life expectancy differential.
I don't want to overstate things here -- there are some clear candidates for things that might have gone wrong with health in the United States in the last couple of decades that we want to look at. But I suspect this is not the only thing we're seeing in this data.
This sounds plausible, though there might be many factors playing into this. Most of Eastern Europe has probably experienced a massive increase in wealth and life expectancy after the Cold War, perfectly lining up with the graph diverging starting at 1990. If you travel around Poland or the Baltics these days, the difference is remarkable. On the other hand, Russia has experienced a massive decrease in life expectancy at the same time.
Couldn't find graph-able stats that'd go back to the 90s or are totaled by Eastern Europe, sadly, but poking around here suggests that several Eastern European states experienced a significant increase in life expectancy between 1990 and 2000, three years for e.g. Slovakia.
The excess murder rate is tiny. The highest murder rate in the U.S. in the last 50 years was 10 per 100,000 (in 1980). Murder rates in Europe tend to be 1 or 2 per 100,000.
The median age in the U.S. is close enough to 40, so every year, murder impacts life expectancy by something like (8/100000) * 40.
(The error from assuming the highest murder rate should pretty much swamp any other inaccuracy in there)
It would explain the emergence of a gap caused by other factors that harm USA but previously canceled out by the factors noted that harmed e.g. Europe.
Undoubtedly has something to do with the fact that patients and doctors are not free to make the best decisions for personal care.
You can actually do better in that regard in a German-style nationalized healthcare system than an American-style quasi-national corruptocracy.
But there is only one way to guarantee it completely and in principle: separation of state and medicine, just as we have separate of state and church and should have separation of state and economics.
> just as we have separate of state and church and should have separation of state and economics.
That's a nice series of words that doesn't really have coherent meaning: "politics" and "economics" are different names for essentially the same thing, the manner in which a society distributes power. You can't separate them -- state action is inherently economic.
That's simply not true. Under laissez-faire capitalism, the state is separated from economics except in that it must tax and spend to maintain a night-watchman state (military, courts, and police).
The only thing that state action inherently is, is coercive. (Though I'm not advocating anarchy; coersion can be moral.)
Some have also suggested that unfavorable US
performance is explained by higher risk of iatrogenic
disease, drug toxicity, hospital-acquired infection,
and a cultural preference to “do more,” with a bias
toward new technology, for which risks are understated
and benefits are unknown.
I know some people who use both the US and the Israeli health systems to some degree, and one contrast I've heard is that Americans (patients as well as doctors) tend to prefer newer, less well-tested (because newer), and more expensive (because still patent-protected and brand-name) drugs even when the new drugs have the same or worse performance than decades-old alternatives. I'm not sure if the health drawbacks of this approach are significant, but the economic ones are stupendous; the newer brand-name drugs can be ten times more expensive than the old ones.
I would love to see a comparison graph from Canada.
The US and Canada are not the same country, but they're similar in a lot of ways. If Canada's graph shows the same drop, it'd be an indication that maybe the problem isn't with the US healthcare system, maybe it's something about culture/diet/environment/etc.
We lack basic access to affordable health care, we drive too much which causes more fatal accidents/injuries, we don't walk enough so we don't get enough exercise, and we eat highly processed foods. Pretty simple.
Universally available public health care, or lack there of. Americans spend a disproportionate amount of their GDP on inflated (private) health care costs, and are therefore more reluctant to seek treatment before conditions become acute.
"perhaps doing and eating what we want (to the extent we’re making choices) is more valuable than lower mortality and morbidity"
It seems more systemic to me. I go to my supermarket and decide to eschew snacks like candy or potato chips for dried fruit or the like. But even the dried fruit has extra sugar added to it. I look at the vitamins and such on some yogurts and there is very little healthy about them. Normal dinner type foods are loaded with sodium, cholesterol, saturated fat etc. Even when one wants to be eat healthy, it can be a trial, because so much food is loaded with junk, even "healthy" type foods.
i don't agree with this, at least for people who can afford it or live in non-food desert areas (you didn't make the distinction in your assertion)
if you walk into a any grocery store, there's fresh/unprocessed meat, poultry, eggs, fish, vegetables, fruit everywhere. you don't need to buy anything that comes in a box or wrapped in plastic or has added sugar or salt or anything.
you don't need to eat anything beyond that selection to be healthy. whether or not you want to go through the trouble of preparing it is another matter.
Most people haven't learned how to use a shopping list? What people are you talking about exactly (emphasis, as I'd like to know who you're describing here)?
I grew up in poor Appalachia. Every single person I knew, understood perfectly well how to use a shopping list, and how to cook. I simply can't imagine who these people are that don't know such things, given my comparison group is in theory low on the education chart.
Anecdotal: I grew up knowing how to cook and prepare meals since I was 10-11 years old or so. It was a complete shock after college to find out that my roommate (that I had gone to school with) could barely boil water.
I just assumed everyone knew how to cook at least basic things because that was how I was raised. He was raised with his mom doing everything for him, so after graduating (meal plans in college meant no need to cook), he literally could barely make toast. For the first 6 months after living together, his dinner usually came from Burger King.
Now I find that people my age (late 40's) and older are often the same way. Somehow they've managed to spend their entire lives eating takeout or microwaved meals.
In my single days, I managed to impress any number of women simply because I made them home-cooked meals. Insane, but true.
I rented a room from a woman who had her mother cook or she ate out. I had to show her how to turn on her own oven. She owned the house, had a beautiful kitchen (open, good appliances, lots of cupboard/prep space) but never used it. Her brother, also living in the house, was AMAZED when I would cook and make my own meals.
It strikes me that "Life Expectancy at Birth" is the wrong measure. I suspect (and would like to see the stats) that the USA has a higher mortality rate below age 40 than other western countries but that it levels out after that.
But is life expectancy the end all and be all. At age 98 my aunt, who was of sound mind and body, was informed she'd probably live to be a 100. Her response? "Oh, God, I hope not." She lived to 102, aware and cognizant to the end.
>I suspect (and would like to see the stats) that the USA has a higher mortality rate below age 40 than other western countries but that it levels out after that
The USA has a lower than average life expectancy at age 65, and the life expectancy has also grown less than average for that group, according to the OECD[1]
EDIT:
>But is life expectancy the end all and be all
I agree there. The same document includes a "healthy life years at age 65" (only for European countries though), but it is arguably a much less objective measurement and hence less useful.
The US median 1st decile hourly earnings are $7.40. Austria, the Czech Republic, Estonia, Germany, Italy, Japan, Korea, the Netherlands, Poland, the Slovak republic, and Spain are all below there.
Australia, Canada, Denmark, Finland, France, Ireland, Norway, Sweden, and the UK are above there.
So I don't think that poverty is causing the US to underperform compared to the OECD mean or median.
If one does that I bet that first decile American scores way lower on the number of hours he can afford to spend in a hospital per year, or on the number of days he has to work for a visit to the dentist.
On the other hand, I think he will be able to buy more over the counter medicines.
Well, it's possible that I'm misinterpreting the parent commenter, but I don't think it's a very strong or interesting statement to say, "I think that lower healthcare outcomes are due to worse healthcare."
I assumed that when dewiz listed "poverty" in a group of confounding variables like "war" or "pollution" (which, by the way, is another thing that the US is probably not particularly bad about) in explaining lower life expectancies, he wasn't trying to use "poverty" as a proxy for "low access to healthcare," so much as something that independently worsens healthcare outcomes even controlling for healthcare access.
(And, by the way, while I don't think that it explains the difference in life expectancies raised by the parent article, I do agree with dewiz that poverty almost certainly has a negative effect on healthcare outcomes, even if you perfectly control for access to healthcare.)
They are different even then. Earnings relate to poverty via the prices of goods. I'm don't know much about economy but after searching in wikipedia I think the term is called "purchasing power parity".
That's true, but the great-grandparent post was already talking about PPP-adjusted earnings, so that aspect was already addressed when I wrote the grandparent post.
I would be curious to see not just the median but the mean. The median isn't super informative in the sense that U.S. is much more heterogeneous / unequal than OECD
In the absence of high infant mortality, it isn't clear to me why median and mean for lifespan would diverge in any meaningful way. In the presence of high infant mortality, the mean would just be lower than the median: how would that be particularly informative?
Median and mean could and most likely do diverge because poor people live significantly shorter lives than rich/middle class people. Europe in general is more equal than the U.S.
The mean would give the same quantity of information but biased (in this case) by the infant mortality rate, which probably should be examined seperately. The median is the preferred statistical standard.
What you are looking for is a distribution of life expectancies per country.
"the median is the preferred statistical standard" - that depends, not sure what this blanket statement means. But yes, you are right, I am looking for the distribution or a sense of it anyway.
I posted this comment elsewhere, but I thought I'd try it in an active part of the thread to see if anyone can answer my question: Do the OECD averages reflect population weighting, or does, say, Belgium count as much as the entire United States?
You'd really want to see something like a lifespan version of the Gini coefficient to assess inequality. Having the mean as well as the median wouldn't really tell you a lot.
One might guess that around 1995, something happened to the US food supply. Maybe the big surge of GMOs (which didn't happen in Europe because they're banned)?
GMOs are not banned in Europe as a whole, but it looks like only Spain have a significant GMO output [1]. Coincidentally Spain has a nice life expectancy, so there doesn't seem to be an obvious correlation (one might argue that Spain might produce but not consume most of it GM crops, which I don't know).
I also wonder if population density makes a difference. An ambulance should take less time to get to you in Manhattan than 80 miles outside of Houston.
{kind=link}
{kind=link}
{kind=link}
Answer: Americans engage in more risky behavior than other OECD members (driving, we also drive worse than some OECD members, etc):
http://www.forbes.com/sites/theapothecary/2011/11/23/the-myt...
http://b-i.forbesimg.com/theapothecary/files/2013/11/Nationa...