>Targeted chemotherapy consists of drugs that are meant to specifically kill cancer cells and not healthy cells.
Putting immunotherapies (like nivolumab) under this category I think will only confuse the reader about the state (and direction) of oncology.
Nivolumab doesn't target cancer cells, it blocks an inhibitory receptor on T-cells, which then kill cancer cells more readily. It's been approved for a wide range of cancer types since it's really a treatment of the immune system:
Approvals to date: melanoma, lung cancer, kidney cancer, hodgkin lymphoma, head and neck cancer, bladder cancer, MSI-H colorectal cancer.
The distinction between targeted therapies and immunotherapies is very important since, aside from different mechanism, they also tend to have very different trajectories of relapse/resistance. Any metastatic cancer is essentially guaranteed to become resistant to a targeted therapy within 6-18 months. Drugs like nivolumab, on the other hand, offer a minority of patients (10-40% depending on the cancer) a chance at durable responses (cancers either cured or prevented from spreading by immune surveillance).
I am being treated with pembrolizumab for metastatic MSI-H CRC (I'm in my late 20s). Last year the cancer rapidly metastasized further, covering my abdomen in tumors. Prognosis was not good to say the least.
It took around 12 weeks for the treatment to "kick in", but at that point tumor regression became rapid. Every CT scan since has shown significant reduction in the abdominal tumors until my last one a few weeks ago; there is no longer any sign of cancer in my abdomen. Overall, it went from "countless" visible tumors ranging from a few mm to several cms each in size, to nothing visible on CT today. o_O
Who knows what the future will bring. I'm trying to be optimistic but I'm also realistic about the statistics here. However, going from my literal death bed where I was in horrible pain suffering for 24 hours a day to quasi-normalcy in a matter of several months blows my mind when I think about it. It did give me horrible colitis (yay for autoimmune side-effects!), but I'll take that over a painful death any day of the week. The colitis is bad enough that they had to discontinue the treatment for a while.
tldr; Science rules. Side effects suck. And a sincere thank you to anyone reading who is or was ever involved in cancer research.
The obvious question is : given all of the facts presented why is a multi-billion industry stuffed with the finest minds and equipment that can be bought or found carry on in apparent defiance of reason?
I see three explanations. First the pharma/cancer industry is a giant conspiracy working against the health and needs of cancer patients everywhere. Second, for some dreadful reason none of the brilliant minds working ceaselessly day and night have noticed these facts so far. They haven't read the studies and have been unable to parse the evidence, data science (counting) to the rescue. Third, there are other facts and knowledge which the author and readers external to the industry are not privy to, possibly because acquiring them required seven years of medical school followed by twenty years of biomedical research.
The premise of this blog post is flawed. Despite the madness of the pharmaceutical industry, we are currently experiencing a revolutionary improvement in treatment.
Essentially nothing interesting, from the patient's perspective, happened between the time that effective chemotherapy combinations were formulated (60s & 70s) and roughly ten years ago.
More recently, however, there have a surge of approvals in immunotherapy which have turned death sentence diagnoses (e.g. metastatic melanoma) into potentially survivable diseases. The 2 year survival rate for stage IV melanoma has increased from ~5-8% to 20-40%. The tools used to achieve this increase in survival are broadly applicable to other cancers and have been achieving gains in survival for lung cancer, bladder cancer, &c. More importantly, immunotherapy research is just getting started and there are lots of promising approaches (personalized vaccines, engineered T-cells, oncolytic viruses, more interesting routes of immune modulation). Many of these approaches seem to synergize. So, treatment has improved dramatically for many indications and looks like it will continue improving. There are some cancers which a patient is still unlikely to survive (pancreatic, GBM), but the industry's output of useful drugs is definitely not stagnant.
Now, the pricing of those drugs once approved is a whole different problem...
I used to work in cancer research and I don't think it's fair to say that we're experiencing a revolutionary improvement. It looks pretty marginal to me. Sure, some cancers (the "easy" ones) are making significant improvements and grinding down on death and recurrence rates.
But most of what you are describing is forward-thinking, not an accurate description of today.
Were metastatic melanoma and NSCLC considered "easy" before immunotherapy? My understanding is that they were near certain death sentences.
I think that the progress so far certainly looks revolutionary compared with the previous few decades. I also agree though that a lot of excitement is related to perceived future benefits.
If startups were making progress this slow on things like self-driving cars, we'd be very underwhelmed. At this rate, we'll all be dead before the majority of cancer treatments are successful.
Technology starts off slow and then, as the base of knowledge upon which one can build expands, it snowballs into daily breakthroughs and progress before plateauing and repeating.
In other words: different industries. Apples and oranges. Do you really think only programmers have creativity and innovation?
Yup, my background is in biophysics but I do software engineering because it's relatively easy. billion-line codebases aren't really complicated to a single cell.
I mean, we've had a small percentage of the planet's human population * 65 years or so to engineer code complexity?
Even given intelligent (depending on the code's author) design vs random evolutionary pressure... every living thing on the planet * billions (/Sagan voice) of years is a long time to compete with.
I suspect that for better or worse, the answer is more prosaic than any of those- the finest minds realize the problem, but no one has any better ideas what to do, so they're continuing on in hopes of getting better results eventually.
It's a sort of categorical issue- we've tried inexact, scattershot methods that are just barely controlled enough to be called "medicine" (i.e., cytotoxic chemotherapy.) Now we're trying "targeted" methods which tailor medicines to effect cancer in known ways (i.e., "targeted therapy.") What else is there? Those two categories essentially cover the whole paradigm of "giving medicine to patients."
(Note, incidentally, that there is other work going on in the field- early detection/screening methods, for instance, or tumor-subtype classification methods, either of which could make the available treatments much more effective in practice.)
I think 4 is a much larger issue. Cancer is hard, and low hanging fruit is easier to find.
Also, adding 4 months of life when you're talking about something 40% of Americans are going to be diagnosed with really is a huge deal. Adding say 1 extra day of life to every cancer patient in the US would be the equivalent of saving ~25 lives each and every year.
It's hard to talk about in aggregate because chemotherapy doesn't have the same effect on all types of cancers.
I went through it. Aside from whatever months it added, it took about 3 of them away because I wasn't doing anything other than barfing, chugging hydrocodone syrup, and sleeping for that time period.
I should also add that I clearly wasn't getting the worst of it. Breast cancer patients seemed to have 6+ months vs my 3+ months for my adenocarcinoma. Also, I didn't lose my hair, finger nails, etc. It was, though, 3+ months lost to nausea, hydrocodone fog, pain, and sleep.
I'll try my best to give my two cents (as someone who has done medical school and works in biomedical research). Your explanations all have some merit.
Having spent time working in/with the research and clinical trial divisions of large pharmas (and their oncology programs), I don't think there is an actual "conspiracy". However, there are certainly circumstances where incentives align (or misalign) such that the pharma/cancer industry devotes resources/time/energy into relatively futile efforts. As brought up in this article, currently we see a proliferation of cancer therapies that have slim (or debatable) benefit in progression-free survival or overall survival. Crucially, because CMS & insurers will usually reimburse the exorbitant prices for these therapies, the pharmas continue to search for, research, develop, and market them. Simultaneously, pharmas will continue to point to the high costs of R&D to justify the costs of therapy. (In some cases those R&D costs are quite exaggerated, but that is another story.)
Since pharmas are constantly trying to balance exploration vs exploitation (i.e. a multi-armed bandit), when they find a therapeutic paradigm that is profitable, a big chunk of the research enterprise & industry ramps up to it: NIH grants, university research programs, startups, etc all start pumping out research and therapies and such in that area. In the past decade-ish for oncology, it has been targeted antibodies/inhibitors: all these -mib and -mab drugs. As this article points out, sometimes these targeted therapies truly do work for some sets of patients/diseases. The progress has been undeniable. Sure, there are therapies which give a few months of progression-free survival at the rate of $100k+/year, and then we find that overall survival doesn't budge. But there is significant hope that maybe if we look at the right subset of patients which the right type of disease, or develop a more targeted and more specific inhibitor, we will get even better results.
Which points us to where a lot of oncology is going now, which is toward "precision medicine". Some of the new cancer therapies are useful only if your tumor exhibits a specific genetic mutation. That is, it might not matter if you have lung cancer or breast cancer or colon cancer -- if your cancer has a mutation in XYZ gene, you should be on ABC inhibitor.[1] For some patients, the results for some of these therapies have been near miraculous. For some, it has not. But again, it gives us hope that there is a lot to be learned, as uncovering tumor DNA sequences has not been cheap or easy until relatively recently, especially since tumors exhibit heterogeneity in their DNA. Another hot area is personalized immunotherapy, as with CAR T-cell therapies, which harvest your body's immune cells and custom re-engineer them to attack your cancer -- definitely not a cheap prospect currently.
So as therapies get over the hurdles of showing "enough" benefit vs risk to get through the FDA, and as payers agree to reimburse for them, once again the research enterprise will increase its resources to these new paradigms. And with all that inertia behind it, sometimes the research field is over-excited about the uncovering of an previously unknown mechanistic link and the promise of new therapies... and we end up a little blind to the crappiness of the clinical studies and actual outcomes. I believe the system can be better. But as of now, the costs and the incentives and the burdens of heavily regulated R&D and the sick patients combine to make it a challenging landscape to work in, and alas that is currently how it works.
[1] One example is microsatellite instability / mismatch repair & a therapy called pembrolizumab, which was uncovered during a trial of patients with advanced colon cancer that was going very poorly, except for one patient who had an incredible response to the drug. Further investigation and subsequent studies demonstrated a link, reported in NEJM (http://www.nejm.org/doi/full/10.1056/NEJMoa1500596) and elsewhere, leading to eventual FDA approval for that indication.
I think the problem in the cancer research community is much the same as the one in the aging research community, which is to say pursuing very inefficient strategies. My theory is that the root cause is similar, which is that researchers and funding institutions will follow a path of least resistance that runs as follows:
- investigate the biochemistry of the disease state in a fundamental research paradigm, fairly disconnected from incentive to build treatments, and very distant from root causes. They work backwards from the end state.
- find new discoveries, 99.9% of which can only lead to marginal strategies, because they are working backwards through proximate causes. If you mess with proximate causes, you are not building cures.
- nonetheless, a healthy dose of status arrives from the applicability of findings, so everyone involved is incentivized to oversell applicability. The researchers are usually less guilty, the institutional support network usually much more guilty (but look at David Sinclair as an example of the inverse).
- then the institutional funding for translational development, that really has no capacity to judge expectation value, and is staffed by exceedingly conservative people who are not going to get fired for deploying funding in exactly the same way as their predecessor, deploys money towards marginal strategies that really only arose as a form of status signaling.
So that something effective happens is entirely a happy accident.
As to where most of the blame lies, I'd say the translational research funding institutions. It is their job to pick good projects, and it should be their job to influence earlier parts of the chain towards higher expectation value research and prototyping. Doing that would be vastly cheaper than the present utter waste of value.
LOL. I worked in pharma/oncology. There are a lot of very smart people, but no risk takers and the smartest people I was schooled with do not work in life sciences research. Research, and by extension pharma, does NOT pay very well compared to most industries. If you are literally 'brilliant' it is a really terrible ROI for you. Additionally, if you are of the type that likes to take moonshots and think outside the box, pharma is not for you (though research in some other areas may be more fitting).
For some reason, every other industry talks about how they need to pay well to attract the best talent. Biotech/pharma/life science researchers talk about how terrible someone must be as a researcher if they care at all about money. It's quite frankly, disgusting.
I get a sense that you're pushing for option 3. It's ... certainly a live possibility. However it does have to be pointed out that the medical profession's record of responding promptly and appropriately to information showing that it needs to change its methods has never been great.
> medical profession's record of responding promptly and appropriately to information showing that it needs to change its methods has never been great.
Why do you think that? Medicine is one of the most data-driven industries out there, and usually very promptly responds to new therapies, etc. Particularly for cancer.
I'm not sure what you're thinking of with regards to this.
I don't understand - what I was trying to say is that deep domain expertise and experience is fundamental to doing this kind of analysis and inference.
>First the pharma/cancer industry is a giant conspiracy working against the health and needs of cancer patients everywhere.
as a former insider, i will tell you that this is not the case.
the real case is not nearly as bad:
imagine two therapies that are in prototyping phase, being tested extensively in hundreds or thousands of tumor-prone and heavily irradiated mice, but still not yet ready for clinical trials in humans.
one of the therapies is cheaper to produce, has one or more cousin-drugs that have cleared the trial process and have FDA approval, and does a worse job at treating the mice when they inevitably develop knots of tumors. the mice who get this therapy die faster, and from the looks of it, they suffer horrendously in the meantime. it affects most of the models of mice in the same way; there are populations which suffer slightly less, but it's still awful. there is a 20% minority of mice that don't respond to this treatment at all.
the other therapy is more expensive to produce-- let's say by about 10%-- but there's no precedent for its use in humans, or if there have been trials in cousin drugs, the trials have not panned out for reasons that many say were merely statistical blips. but in the mice, it's a winner-- they die slower, and don't seem to suffer nearly as much. in some of the mouse models, it's an even bigger winner, and can be curative. and in a few of the mice, it doesn't seem to be effective at all, but this is a small minority-- let's say 5%.
which therapy does the pharma company push forward into clinical trials, and which does it shelve?
the answer is that neither are shelved, but the first therapy goes to the clinical pipeline first, which puts the second therapy at least a few years behind it before hitting the market, assuming it clears trials and the FDA, which it might not.
the risk of the superior treatment's failure is only tolerable by the pharmas if there's a recent success in hand.
this is why patients get shafted in the short run; their suffering is irrelevant to the risk of drug development as far as the pharma execs care.
the first drug will clear the clinical trial process more reliably, which means that it'll get busy treating patients faster, which means that it'll be a moneymaker faster-- even if its side effects make it a second or third line of treatment right out of the gate.
this leads to having a lot of shitty drugs that aren't very effective, but they're better than nothing, and they're probably better than what came before.
then, a few years later, we see the wonder cures. the wonder cures exist in the same therapy ecosystem as the shitty drugs, which now have a few more years of familiarity behind them.
there's one more wrinkle: the drug company doesn't want its drugs to be competing with each other. so the original shitty drug goes back to the mice and likely back to the clinical trials for a different use case, which it gets approval for-- viola, a "new drug" for cancer.
so the pharma companies save lives, often miraculously. as a former scientist, i am proud to have contributed to that.
but it is the nature of the pharma companies to serve humanity's purposes very poorly as a result of the financial incentives they face.
> Its results are distinctly unimpressive... So far as I can tell, where there has been improvement in cancer mortality since the 1970’s, it is mostly due to people smoking less, early detection of some kinds of cancer, and adjuvant (cytotoxic) chemotherapy, not to targeted chemotherapies.
I'll just add this quote for a starting point from such abject failure, "The first step towards wisdom is to call things by their right name." -Confucius
"what's cancer?", "how do you fix it?", don't ask them.
The steady 'progress' is not what it seems. Improved and earlier detection of cancer means that a patient will survive for significantly longer after the detection past the 5 year mark. Several decades ago the patient would die relatively quickly between the period of detection and within the 5 year period.
As one of the posters ( reasonattlm )pointed out,cancer can be regarded as one of the diseases of aging. To kill cancer cells will not improve things beyond a point because the body will produce more. I would speculate if detection methods we sufficiently sensitive, we would _all_ have some cancer cells within us. It is a matter of degree.
Summary: Except of a few types of cancer, the treatment has not improved the outcome for cancer patience during the past few decades. Also remember: lies, damn lies and statistics.
My sources: A non-mainstream cancer doctor ( but is a conventional MD ) who was widely regarded as a quack, by the mainstream medical community. Heresy is not tolerated well.
> Part of this is due to the fact that many of these are drugs for refractory or late-stage cancer; this in turn may be due to regulatory or medical-ethics issues that make it hard to directly compare a new drug to the standard-of-care old drugs.
My best friend's younger brother is currently dying of sarcoma. I think it should be illegal to give therapies (and false hope) which are proven to extend agony and proven not to extend overall survival. Meanwhile, studies of new therapies must be performed on relapsed patients with hardened cancers. As long as this is true, the rate of discovery of effective therapies will remain staggeringly low, and the rate of human suffering from cancer staggeringly high.
It's easy to blame regulations, but in my opinion they are ultimately a consequence of our inability to speak honestly. People I've known all my life, through thick and thin... yet it seems impossible for us to acknowledge the truth of his treatment: progressively increasing suffering and death, at tremendous financial cost to his family and society.
I recently forced myself to break the ice a bit in a conversation with a mutual friend. It was harder than I imagined but went better than I thought it would. Paul Erdos had a way of talking extremely honestly about things... I tried to channel him a bit. I encourage everything to think hard about breaking the status quo of discourse about cancer.
I'm left wondering whether, if I get cancer, I will have the ability to choose experimental treatment in lieu of "protocols" which are proven to be unsafe and ineffective. (If anyone has advice on that, I'd like to start getting a plan together.)
Background: My parents were both pharmaceutical chemists. My father is named on over 40 patents. I invest in pharmaceutical and "biotech" companies with a focus on new cancer therapies.
"I think it should be illegal to give therapies (and false hope) which are proven to extend agony and proven not to extend overall survival."
I used to agree with you, emphatically. Now I'm not so sure.
I had a bone marrow transplant 30 years ago. At the time, one year mortality was 95%. Let's just say it was hard, both physically and mentally. And the doctors absolutely lied by omission.
I see that look of hopeful desperation in new patients every time I go back for a checkup. No doubt patients (research subjects) are being exploited.
But...
Whereas I was a boy in the bubble, similar treatment today is practically an outpatient therapy.
Like a comment upthread, one of my bffs was diagnosed with terminal cancer, qualified for a clinical trial for immunotherapy, now three years later is "cancer free".
Seeing how far we've progressed, now I think our sacrifices were probably worth it. I'm certainly less angry about it.
In my anecdotal experience, giving patients the brutal facts about experimental cancer treatments doesn't shift their decisions much. Regardless of the exact odds, some people are predisposed to fight long odds with painful treatment, and some are predisposed to stop fighting and optimize quality of life. Both choices are legitimate and it's not worth bending the truth one iota to try and get more research subjects (or to bend it the other way to avoid "false hope").
Most lying in this context is driven by the speaker's (partially unconscious) desire to avoid short-term social tension.
Thanks for sharing your story. BMT is a surgery though, and surgery is always experimental in a sense, and has been improving at a satisfactory rate in general. Drugs are a little different. Great to hear about your friend. A close friend of mine died last year of cancer while enrolled in an immunotherapy trial. He wasn't enrolled until after he'd failed two rounds of conventional treatment, and I wonder if it might have been better to do things in a different order.
Bone marrow transplants are chemotherapy (and maybe radiation treatments) to kill existing bone marrow and then infusion of new cells into the bloodstream. It's not a surgery as such.
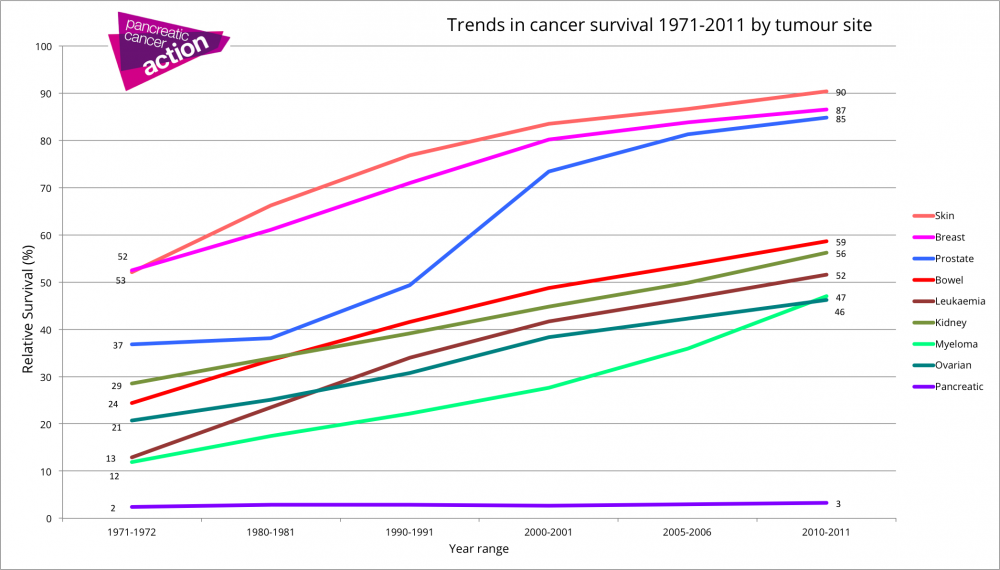
Here is a nice figure on cancer survival changes from 1971 to 2011[1]. The writer is correct that not all of this improvement is down to newer drugs - a lot of it is down to better 'supportive' management - recognising side effects of chemo, keeping on top of transfusions, having cancer centres where all of this can be coordinated, having specialists (oncologists) managing the disease etc etc. For example, the survival of acute myeloid leukaemia has improved dramatically since then, but our treatment has remained the same two old-fashioned drugs.
Also the writer lumps chemo drugs into two categories - cancer chemotherapy, and targeted therapies. That is probably not a good way to look at it as iskander has already mentioned re: immune checkpoint therapy, which is quite different. Other categories include:
* small molecule drugs (not antibodies, target a cell metabolic pathway)
* adoptive cell therapy - grafting antibodies to killer immune cells etc etc...
Progression-free survival isn't as good a metric as overall survival - that is true. It was brought in as a replacement for some other indicators, such as relapse-free survival, which ignored everything (including death due to treatment) except relapse. Progression free survival doesn't let you get away with that. Some diseases have been changed massively by treatment. CML used to have an overall survival of around 5-7 years, it's now so long we can't really measure it since imatinib was brought it. Obviously people do die of the disease, but we don't know what the average life expectancy is because they are doing pretty well. To introduce new treatments in this disease you're going to have to use another metric apart from overall survival.
this is strange since I watched my mother take medicine and survive (trial-to-trial) for over ten years without any traditional chemotherapy, which she wanted to avoid at all costs. A clerical error meant she missed the next trial and.. anyway that was that.
A friend's dad currently has stage 4 lung cancer and has been taking a daily pill for over two years now and just surviving without any of the traditional chemotherapy issues.
These pills are amazing but I guess your luck eventually runs out.
I'm a bit surprised that we're only looking at the results of targeted therapy in late-stage cancer. It seemed apparent to me from the name that targeted therapies were supposed to be less toxic, so they could be used in patients who weren't effectively dead, i.e., in earlier-stage cancers. Late-stage malaria and tuberculosis have terrible survival rates, and those are diseases we're supposed to be good at treating.
Enjoyable read. Anyone know if she did a similar research review of concomitant temporary fasting during the pre-application and treatment periods of chemotherapy? Her blog is not searchable and a domain-specific Google search for relevant terms didn't turn up anything.
Luckily, most WordPress/SquareSpace blogs give you a link to a search page, or a search bar directly, on the 404 page: https://www.sarah-constantin.org/search.
> (Normally we associate decentralization with freedom; but consolidating authority in a small number of people rather than a bureaucratic process can make it easier to get things done quickly and iterate.)
I would hardly call 'bureaucratic process' decentralization.
I have a close friend's mother with lung cancer that is currently being treated with an experimental drug. After reading the "no difference" multiple times I am not too optimistic. I do not know which drug she is taking but :(
Caution: etymologically-oriented answers generally miss important nominological / nymological / onomatological / onomastic foundations. This namespace is a "synthetic" social construction. It has interesting "quirks", "gotchas", and "zingers".
{kind=link}
{kind=link}
Putting immunotherapies (like nivolumab) under this category I think will only confuse the reader about the state (and direction) of oncology.
Nivolumab doesn't target cancer cells, it blocks an inhibitory receptor on T-cells, which then kill cancer cells more readily. It's been approved for a wide range of cancer types since it's really a treatment of the immune system:
https://www.drugs.com/history/opdivo.html
Approvals to date: melanoma, lung cancer, kidney cancer, hodgkin lymphoma, head and neck cancer, bladder cancer, MSI-H colorectal cancer.
The distinction between targeted therapies and immunotherapies is very important since, aside from different mechanism, they also tend to have very different trajectories of relapse/resistance. Any metastatic cancer is essentially guaranteed to become resistant to a targeted therapy within 6-18 months. Drugs like nivolumab, on the other hand, offer a minority of patients (10-40% depending on the cancer) a chance at durable responses (cancers either cured or prevented from spreading by immune surveillance).