Based on Diamond Princess data, where almost everyone was tested, the lower bound of COVID19's IFR (Infection Fatality Rate) should be > 0.5% for many/most countries.
This uses a data source independent from what the paper uses. Here's the calculation...
Current Diamond Princess' CFR (Case Fatality Rate) is at 11 deaths / 712 infected = ~1.54%. Ten more are in serious/critical conditions, so it could increase.
Since testing in DP was almost universal, IFR ~= CFR.
Assuming no one in other age groups/health conditions in a country of interest dies (unrealistic) and everyone from Diamond Princess who is in severe/critical condition recovers (optimistic), population's IFR would be = 1.54%/0.3 = ~0.51%.
Also, cases from Diamond Princess have received good care. If the healthcare system gets overwhelmed as has happened in many places, population's IFR would shoot up to multiple times as high.
Thus, 0.5% is a lower bound for COVID19's IFR, unless a better treatment protocol/medication is invented. Alternatively, if there are successful measures to shield the elderly from getting infected, a region's overall IFR could be lowered.
DP excludes the extreme elderly and sick. Remember, people in nursing care don’t go on cruse ships. Further, it’s expected to see additional deaths. So, such simplistic estimates are completely worthless from their data.
What it does do is provide estimates of the rate of infection vs obvious and extreme symptoms. China’s CFR is over 4% and rising, but it’s known that they missed a huge portion of the total case load.
PS: Further to estimate for the US population you need further adjustments. China has a younger population than the US with only 10.8% of the population being 65 and older, but they also have more air pollution etc.
> DP excludes the extreme elderly and sick. Remember, people in nursing care don’t go on cruse ships. Further, it’s expected to see additional deaths. So, such simplistic estimates are completely worthless from their data.
My estimate above assumes that DP's demographics & health conditions represent >=30% of a country's population and it is a lower bound so additional deaths don't affect it.
Your paragraph quoted here does not negate the logic behind the estimate since "the extreme elderly and sick" and those in nursing care can easily be included in 70% of the country's population.
Calling something a minimum does not make it useful. I can find a minimum bound by taking the total number of deaths divided by total global population. But, while true that’s a worthless bound.
Also, if you’re using passenger demographics then you should use the number of passengers infected excluding the 145 infected crew average age 36.
The goal of establishing a lower bound is to inform decision-making. A lower bound of 0 is trivially true and doesn't help decision-making. A lower bound of 0.5% rules out some policy options, though -- in America, it means over a million people would have to die to achieve herd immunity, which is probably unacceptable to political leaders.
The higher the lower bound, the more policy options can be ruled out, and hence the more useful the bound.
If you know of a lower bound that's higher than mine, based on as/more reliable data, you should mention/link to it. People are doubting the Lancet paper based on data source (I don't have a strong opinion on that), so this bound based on a different source of evidence should provide additional information for policymaking.
Your lower bound based on the population of earth is clearly not it.
Second your using both passengers and crew numbers to hit 712, but 145 of those where crew average age 36 and 567 occurred in passengers average age 69. Thus the demographic estimate of 30% also low.
Finally, for accuracy you need to adjust for the healthier than average population receiving better than average care. But, that’s more debatable.
You can make adjustments and get better estimates with more work. You are welcomed to and let us know the results.
My point is to invalidate some wildly optimistic estimates like 0.1-0.2% fatality rate which is still getting spread around. With some adjustments on my model, the point would still stand.
“All models are wrong, but some are useful.” —- George E P Box
China is also lying about their numbers. They quarantined late, had a potluck of 40,000 people in Wuhan, let Wuhan people travel all over, then had hundreds of millions of people travelling over Lunar New Year.
Instead of the expected rise in cell phone customers, there was a 21 million customer drop. You'd expect stagnation or even a rise as most other forms of communication were shut downn.
In case of China it is helpful to see the breakdown of in-Hubei (epic-center where lockdown enforced after widespread infection) / outside-Hubei. In Hubei CFR is around 4.73%, outside Hubei ~0.86%. It roughly shows how many cases they missed.
Obesity plays a big role in Covid-19 deaths. 33% of Americans are obese, and 65% are overweight. There's a possibility that more obese people take cruises--it fits their lifestyles (unlimited food availability, and they don't have to move much). So the DP data may be tempered by more obesity even though it has less extreme elderly.
Also many of the crew got infected. So the amount of viral exposure may play a big part. People who had to come in contact with dozens of infected individuals every day may be the most vulnerable. This doesn't bode well for retail grocery workers.
Of the 712 DP infections, 145 occurred in crew average age 36 and 567 occurred in passengers average age 69. Far from every passenger was obese and few crew where obese. So, I doubt obesity was that far from US norms.
Anecdata: I've taken three cruises over the last twenty years, and the obesity rate on those was an order of magnitude higher than what I see in my everyday life as a coastal yuppie -- the only other place I've seen that many people who are that fat was at Disney in Orlando. But America as a whole has a way higher obesity rate than what I see normally, so cruises might just be representative of the country in general.
Also, if the theory about BCG vaccination having a beneficial effect turns out to be true, USA never used BCG whereas China and India did (and UK between 1953 and 2008).
Testing may be inaccurate to up to 40% of cases. Not only because the tests are faulty (less likely), but because the virus is not present at the collection spot all the time (more likely) especially if the virus has entered but not yet multiplied enough. It is highly likely based on how this spreads that every single passenger has it right now.
Also, these ships may have a much higher death rate due simply because viral load may be much higher (another factor we are still guessing it). If the body gets a strong dose when the infection first happens, the anti-body building process may not be fast enough to fight it off.
If the body gets a very small load, it is more likely to start combating the virus, perhaps at a rate slower than replication rate, but eventually it can kill off even a major infection as long as it entered slowly.
For a country with ~10% over 70 years old, and assuming infection fatality rate of ~6% among those, then IFR would already be 0.6%. So suppose that what you've read is the current statistics, it does not contradict the calculation above.
> For a country with ~10% over 70 years old, and assuming infection fatality rate of ~6% among those, then IFR would already be 0.6%
That's assuming equal or greater rate of infection for people over 70.
That is, given 1000 people, 100 would be over 70. If 10% of them get infected (10 people), but 50% of younger people get infected (500 people), your IFR could be much lower.
We have some data on the age distribution of severe cases, but asymptomatic cases are virtually untested at this point, and are probably (? may be?) going to shift the distribution toward younger people (right now, we see more cases for older people, as well as more severe cases, because severe cases are more likely to be tested).
You're right. My hypothetical above was for a very limited context of answering its parent post only and not meant as an inference regarding the IFR for other age groups.
Everything you've said here is consistent with the parent comment. You've got a lower bound on the infection fatality rate of the whole population, given the usual distribution of ages. But you've only got an upper bound on the fatality rate of a population artificially chosen to have an age distribution that includes nobody over 70. (Actually you do have a lower bound but it's 0%.) That is relevant to anyone who's under 70 and is asking about a population who's only member is themself.
My calculation above simply does not answer the question regarding IFR for each age group. It is based on overall statistics from Diamond Princess.
The sample size from DP might be too small to answer the question, esp for younger age groups with lower IFR. We might need to look at data from South Korea and Germany, for example, to estimate those. It would require a more complicated model since testing in any country is not universal.
You’re right, my mistake. Doesn’t this still assume even distribution across all ages? With current testing (at least in the US) people >=70 are more likely to have other conditions which complicate infection and therefore more likely to be tested.
> Based on Diamond Princess data, where almost everyone was tested, the lower bound of COVID19's IFR (Infection Fatality Rate) should be > 0.5% for many/most countries.
No, you can't compare a country's likely outcome to that of a cruise ship. On ships, the virus propogates very differently and the viral load will likely be much higher in infections due to constant contact while onboard. When viral loads are higher, the severity of the disease and mortality rate are also much higher [0].
That's a good point. It depends on how many infections on DP occurred after passenger isolations & mitigation measures, which would also lower viral load. I'm not sure we have that data. They stayed on the cruise for a long time. A Japanese expert went on the ship to examine the practice and he was very concerned of further infections.
Viral load from infection on DP would be quite close to those living in the same apartment/house/nursing home. In a country with multi-generation households, the viral load could be similar, unless measures are well taken. In other countries, the viral load would depend on how well the elderly are shielded from infection.
Yeah, two things worry me about Covid: the fact that the percentage is non-negligible even for young people and that the variance between case severities is high, even to the point where people think they don't have it but do.
The test they gave only tests for live viral load. It's possible there were cases that were asymptomatic, the immune system took care of it, and when tested they showed no virus, even though they had it.
The only real way we can know for sure is giving mass random antibody tests to a population.
> DP's demographics is representative of > 30% of population of many/most countries.
Regarding age maybe but what about health? Could there be a higher representation of people that have a long illness and want to go on a cruise before they can't?
Let's presume this death rate is accurate to within an order of 2- 1.33% to 0.33%. We can use that to do some interesting estimates on the true infection rate.
https://www.worldometers.info/coronavirus/ (trust it if you like) says that the USA has (as of 2020-04-05T15:13:00Z) had 9,119 deaths- and I was going to say 8,486 but I refreshed the page and it jumped to 9,119 because of course it did.
9,119 / 0.33% = 2,763,333 infections.
9,119 / 1.33% = 685,639 infections.
But, we also have to consider that death isn't instant- so add in everyone who became infected in the last 5-10 days. That'll be a bigger number. The reported number of infections because of limited testing is 320,828.
I think it's not unreasonable to say that probably 1m Americans have now been infected by this virus. And the longer ago this comment was made, the more likely that estimate is correct.
Edit to add: I trust the number of deaths more than the number of infections because it's easy to say "don't come to the hospital to get tested if you don't need to" but it's hard to say "let's pretend that dead body died of something else".
> it's hard to say "let's pretend that dead body died of something else"
Pretends is a strong word. How many people who died of pneumonia during the last months did die of covid-19? It's not possible to know unless you test every dead person, even those who were never hospitalised. Respiratory infections is not an uncommon cause of death with the elderly. Not every country have tested exhaustively for this, which need not be of ill intent.
One article I read recently brought up a topic on how unreliable testing and confirming the dead are currently that to get a more accurate count we should look at year over year deaths. This could be broken down to compare deaths in a county the last x years in March to this year.
To me it makes sense I suppose, yoy is a pretty common tool. But I'm just a reader, so perhaps it is not correct
The variations in deaths between years is so large (over 30k deaths difference, sometimes up sometimes down) that year on year comparison may not be meaningful. You could just twist the data to prove any point, even that covid-19 reduced deaths.
That's a really fair point, but I suspect for the moment at least the dead or very seriously ill are all being tested. Most deaths are happening in hospitals, for the moment.
My father, for example, is currently in the hospital for something other than Covid-19 but as soon as he got a mild fever he was rushed into isolation and given the tests for it. (He does not recommend the up-the-nose test at all.)
They are doing that as well. Just a few days ago I read a mortician was told that 3 dead had coranavirus but only the death certificate of only 1 mentiond coranavirus. They are not testing many of the dead so the deaths are being undercounted by a large number as well. This is not just a Us problem but in many other countries as well.
the problem with relying too much on death is that even trying to be accurate if the system is overwhelmed they will not spend time, resources and precious test on a death body. This is not speculation, it's happening in China, Spain, Italy (sorry can't remember the source)
But how do we define mortality? This is not an existentialist question, it is just that somebody infected needs one or two weeks to die. Closer to the truth might be deaths/infected-10days-ago and that will be a lot bigger.
If instead one divides only those that “completed the process” meaning dead/healed, events which also happen in a more similar time frame, that ratio is also a lot higher.
TLDR: I need help understanding what a “death rate” should be.
CDC says USA deaths are at 6,500 as of yesterday 4th April [1]
Considering they were reported in the news[2] as 600 on Tues 23rd, 1000 on Thurs 25th, 2000 on Sat 28th, 3700 on Mon 31st, and the infection rate increasing steeply, to have “only” 6500 or 9100 a week later is quite flat.
Yes deaths lag infections, but on the same CDC page the total infection count graph has only been increasing faster over this time, from 80,000 to 260,000.
Doubling every three days would become 7-10k dead midweek, 15-20k dead by now, this weekend. (That’s the reported infection rate in NY and Michigan, by the media), and it’s half that or less.
Has the death count slowed significantly this week? A Phantom of vague rounded numbers?
The US death rate is the sum of a bunch of time-lagged exponential curves. For instance, CA is 2 weeks after NY. Numbers from individual states are more informative (but have similar issues for big states):
I believed we were at the 1M level about 3 weeks ago. I think we're at the 50 - 100M level at this point, but we won't see those numbers, ever. We will probably see about 5-10M US infections in 3 weeks, which account for the extremely small percentage of people getting tested, and at that point (in 3 weeks) the number of actually infected people will be at least 40% of the US population. I think at that point it will also have waned quite a lot, but we're just playing catch up with the vast numbers of people that are already infected. For a lot of people there's easily hideable symptoms and people are likely going to their grocery store jobs anyway.
That's ridiculous. We're only testing people with severe symptoms and telling everyone with minor symptoms to stay home. We're not testing anyone without symptoms. And the positive test rate is 18.6%.
Why is anyone interested in age independent of comorbidities? Yes - age and comorbidities are correlated. But wouldn't it be more helpful as an actionable guide to have statistics for death rate vs. comorbidity rather than, or in addition to, age?
Fatality rate with treatment is basically irrelevant at this point. We need to know the hospitalisation rate, the ventilation rate and R0 under different levels of lockdown. The actual rare of deaths will depend on these numbers, 0.66% is just the baseline.
Italy is doing a reasonable amount of testing and has more like 10% death rate. Could there be 15X more infected in Italy than detected? Or is it that they have mostly old people catching it? Seems like a large discrepancy either way.
Yeah Italy missed a lot of cases with their testing, which makes it seem higher. Spain also.
If you look at Germany, South Korea you see a much lower death rate, but they also have younger populations. In this case you want the min, not the max or the average, because the death rate of the virus should be fixed. The lower the rate just tells you how effectively the country did their testing, and thus how accurate the denominator is.
What complicates that greatly is the fact that the age of the population matters a lot. And Italy has one of the oldest populations. Countries in Africa with very young populations would expect a much lower death rate - complicated again by their relatively poor population and health systems and incompetent and corrupt governments.
Median hides a lot of information. What you really want to know is how many people over 70. Still Germany and Italy are almost equal there at 20% over 65. South Korea is about 13%.
Given it's so close between Germany and Italy, testing probably accounts for the majority of the difference.
Italy had CFR 2% before their intensive care capacity hit the wall and advanced triage kicked in. They have also very tangled households where old and young live together and they are extremely social but I think you may say the same about Chinese (perhaps somebody with better knowledge can extend from this). The same happened in Spain.
I think the CFR we see is mix of multiple things. Testing protocol (who gets testes - every possible case, only seriously sick etc), social structure (household structure, standard social behavior), demographics, chronic illnesses, health care capacity.
I have observed two patters. When there are low amount (~20%) of elderly among the infected and health care capacity is not reached then CFR can be very low <<1% (Germany 02.% in the beginning for long time, Norway 0.5%). When there the number of elderly reaches is > 50% then the CFR will be order of magnitude higher (Italy, Spain in the beginning).
When health care capacity is exceeded then CFR% will rise about 5 times (Italy, Spain).
It's definitely possible that there are more infected then reported. The issue is Italy is testing only people who are suspected to be sick in the first place.
Most of the people who got covid, are asymptomatic thus they probably won't be tested and added to the count.
This means that 10% is taken from a population of people who are both sick and symptomatic.
Since China is testing asymptomatic people as well, they should have a more precise ratio.
Italy is probably not testing anywhere near as many people as they optimally should or rather the disease has outpaced their ability to test. Add in a collapsing medical system and the end result isn't pretty. Unless you're on death's door I assume there's little point in someone taking up the system's time to get tested in Italy.
As a comparison, Germany has a <2% fatality rate and has tested more people than Italy.
"As a comparison, Germany has a <2% fatality rate"
Germany's good numbers may not hold.
20 days ago Germany had 7256 cases. Italy had 27977.
10 days ago Germany had 37307 cases. Italy had 74383.
0 days ago Germany had 96076 cases. Italy had 124629.
The point being that Germany saw the outbreak take hold considerably after Italy. Italy had a very low original death rate as well -- approximately 2% weeks into the outbreak. This virus takes weeks to kill most of its victims.
14 days ago Germany had a death rate of 0.375%.
7 days ago, Germany had a death to case rate of 0.75%.
Today it's at 1.5%. It has increased every day between.
The fact that Italy is a hyper-social society, while Germany, at least from my probably wrong foreign view, is quite the opposite, probably changed the path of the disease, accelerating its spread in Italy.
Yes, as the infection spreads testing becomes overwhelmed and the apparent fatality rate goes up. A recent trial found that in one German town the actual fatality rate was 0.37%. They did antibody testing so they knew everyone who had been or was infected.
I am not sure if it’s even possible to give the fatality rate before everything is over because we don’t know if an infected patient eventually dies from the disease with a long delay. This is why I totally expect a growing fatality rate now.
The developing world will be devastated. Over 3B people, with marginal healthcare systems, and fragile governments. It's not too far fetched to see 15m people die from this. And possible a magnitude higher. Not to mention all the knock on effects.
i really think herd immunity is their only hope but govts are too scared to not do a lockdown which is insane give none of them any social safety nets from the poor and a large part of population earn their food on a daily basis.
Germany tests a lot more, and started testing earlier. Italy got overwhelmed, for a very long while only tested suspected people (those that have fairly severe symptoms)
It happened, because it just now hit the German seniors homes. It didn't before. In Germany seniors do live in special homes, seperated from their children. Unlike Italy or Spain.
Also beware that the Italian IFR for the bi-yearly flu peaks is extremely high, 1%. (2014 being much worse than this year with the new flu). The current IFR looks also to be in that ballpark.
From what I've read the lethaliy is higher both because they can't test enough people (meaning that they tend to only test the more severe cases) and also because the hospitals were overwhelmed (meaning they can't provide appropriate treatment for everyone).
Germany also have masses of spare ICU capacity. To the point where they will take so-far-mild cases to hospital at day 5 (the point where you may deteriorate) so they’re ready if they do. Obviously that improves your chances a lot!
China only counts certain cases. For example if you had covid and retest positive later it doesn't count unless you have physical signs. Your death doesn't count unless it's in a hospital. Many barriers are in place to prevent you from being admitted.
That's your assumption with Chinese CDC number, which is true. But Chinese researchers and MDs also publish papter on Lancet/NEJM/medrxiv which sometimes contradicts CDC's reports, which I think is much more believable.
They can't get accurate numbers because patients aren't even allowed the test, allowed to be admitted to hospitals. While the researchers will be able to retrieve some facts they won't be able to count those that never made it into the system.
It is based upon Chinese data that we know is effectively junk, to which they add pure speculation: The methodology for determining those infected but not symptomatic is complete guesswork. It is invented rationalization atop garbage data.
A few countries are starting mid-sized randomized studies to look for antibodies in the general public and that will give us a much better idea of the scope.
To which it should be noted that already there is fake news spreading making broad claims that they already discovered XYZ (saw one atop Reddit).
I realize there are China sympathists on HN, however it is widely known and acknowledged that China has been very deceptive about the scale of the outbreak and the number of deaths.
Please make your substantive points without flamey swipes about "China sympathists". Solid factual critique is welcome regardless of whose sympathies it favors, but when people start planting little swipes and booby traps against the other side, it evokes worse from others, and down we spiral. That's called nationalistic flamebait, and if you're going to post on a controversial topic, you need to clean your comment of any of that so it can be a good contribution to discussion.
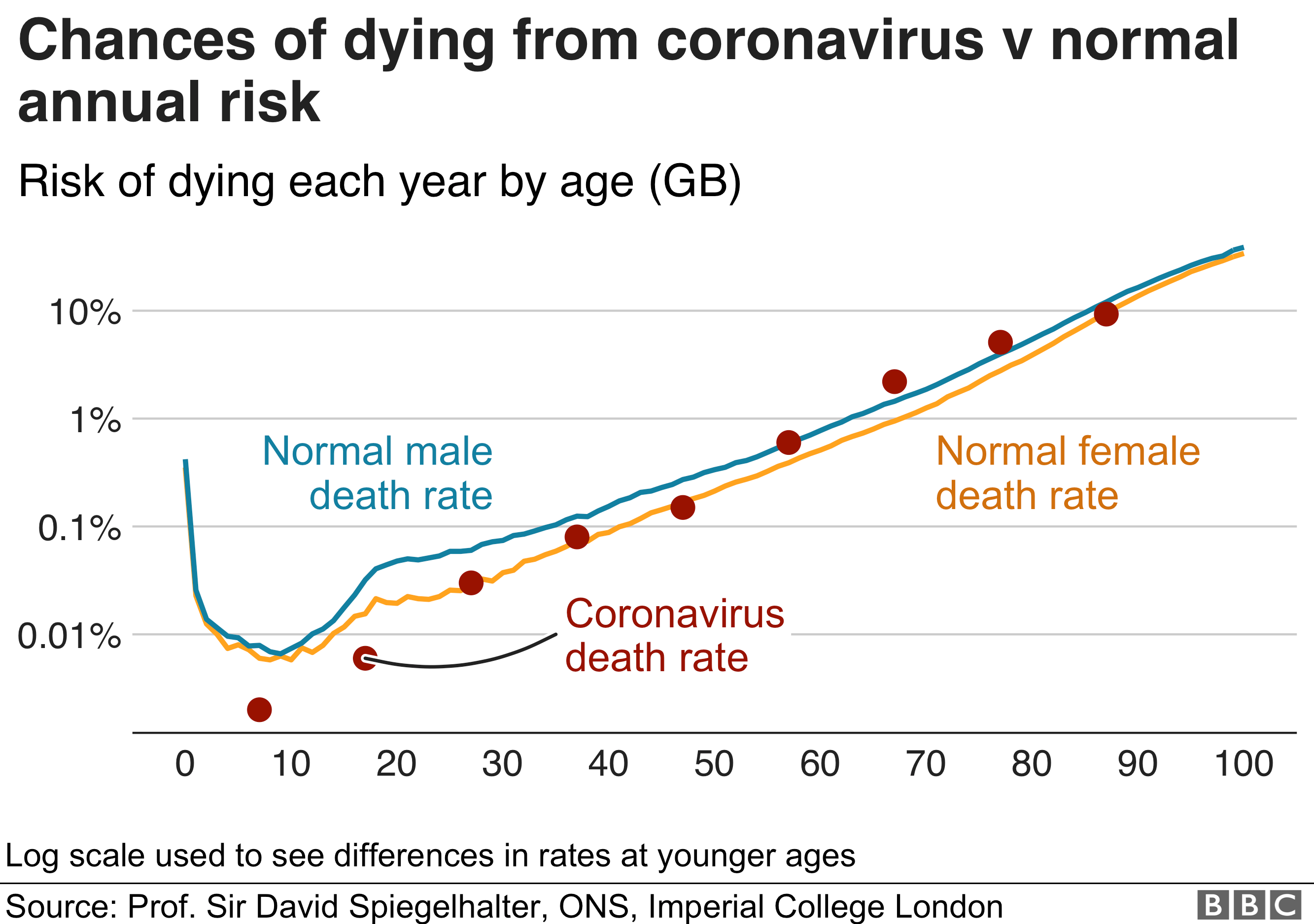
Your death rate is roughly double your 10 year mortality. So if you're in your mid 30s and your risk of dying at any time over the next 10 years is 0.2%, then your risk of dying if you get Covid-19 is 0.4%.
> It reported that 0.04% of 10-19 year olds would probably require hospital care—as would 1.0% of people in their 20s, 3.4% of people aged 30-39, 4.3% aged 40-49, 8.2% aged 50-59, 11.8% in their 60s, 16.6% in their 70s, and 18.4% of those over 80.
This is quite a bit lower than the 20% number that people have been using for while.
Estimates are in the last column of Table 1 (page 5).
These seem roughly in line with CDC estimates for the US, see e.g. the first chart in this article from 6 days ago which compares flu mortality rates with COVID-19 per age bracket:
To the (many) commenters here dismissive of the paper -- because in a "foolish" way it relies on "doubtful" "suspect" "junk" "Communist" Chinese data making it "not worth the paper it's written on" (all quotes from other comments here) -- the authors specifically address "adjusting for demography and under-ascertainment". The fact that they came to results similar to US data, as long as their methodology wasn't cherry-picked, would seem to be a good sign.
And remember -- The Lancet is one of the most prestigious medical journals in the world. They're not going to publish something "junk".
This isn't a peer reviewed paper. It's an extremely brief summary piece based upon a complete absence of evidence and then suppositions.
And to what the guy above said, the Lancet infamously published Wakefield's since debunked repeatedly claim that MMR vaccines cause autism. A paper that has literally led to many deaths.
That was a one-off that made international headlines because it was a rare event. You'd generally trust stuff published in the Lancet; it gets thoroughly checked.
This is work done by leading researchers in the field, in a top-class journal. I'm going to trust it over random allegations on HN.
It was an incredibly damaging one-off that has killed children. Clearly the vast majority of their work is worlds better than that, but I was replying to the appeal to authority that demands respect and belief for a work that itself purports to be nothing more than a very rough estimate.
Nonetheless, this piece isn't "thoroughly checked" because there is nothing to check. They took the deficient data from China and added suppositions to it. It's neat, I guess, but meaningless.
This paper is not being taken as authoritative anywhere. No one is making policy decisions on it. Zero ground-truth is changing because of it. Because it's a cursory, superficial guesstimate (that is literally the most accurate word) just to appease curiosity.
"They have no motive to supply false data, and lots of reasons to make it accurate."
They are working with garbage data. They know this. They admit it. Then they rationalize that they can invent real data out of it. And as an exercise that is okay -- they state exactly what they are doing with very limited, poor data. They haven't claimed it was more than it is.
This is not the canonical statement on death rates, and compared to actual emerging data is completely irrelevant.
"are also authors of the Imperial study that has significantly influenced the UK government response"
The catastrophic and flippant UK response? The one that thought they would obtain some "herd immunity" by doing nothing, and then realizing cases were skyrocketing mimicked what other countries were doing? That UK?
> The one that thought they would obtain some "herd immunity" by doing nothing, and then realizing cases were skyrocketing mimicked what other countries were doing?
Yes, that one. This was the study that convinced the UK government to change course from the original unrestrained herd immunity strategy.
It relies critically on estimating the number of asymptomatic cases. To do this accurately you need either the PCR test to report a positive for a long time after contraction, or you need a serology-based test.
They are basing the asymptomatic case % from the Diamond Princess data and assuming that all people who tested positive where the only ones who had cornavirus. Is this warranted?
Has anyone seen any data on the period of time after contraction during which the standard PCR test will return positive?
For reference seasonal flu is around 0.1% and also increases with age, so Covid-19 is at least 6X as deadly as the flu.
This article also doesn't mention lasting effects. I have seen reports of people with bad cases being left with lung damage but I have seen no statistics on this. Everyone is focusing on mortality so I wonder if they're bothering to collect this info. If it leaves a lot of people with pulmonary scar tissue that's a big deal.
> If it leaves a lot of people with pulmonary scar tissue that's a big deal.
I think it's simply to early, maybe in the next 1-3 years you can have a more precise picture. We don't know if people with pulmonary scar tissue will end up recovering, or if it's permanent damage (from what I've seen it will depend on many variables, age being one of them).
Even for mortality rate, we need to see this through to collect unbiased data from USA and Europe.
> This article also doesn't mention lasting effects.
The problem is ARDS: Acute Respiratory Distress Syndrome.
Some portion of the people who enter the ICU develop ARDS and typically need to be put on a ventilator. A large percentage (~40%) of those people die, and the many of the rest may be left with lasting effects.
Here's a great video detailing the mechanism of ARDS:
Looking at current US data I see Covid-19 deaths almost exactly 6x influenza & pneumonia deaths. And that's with flu being endemic but Covid-19 still not having done a lot to areas with little international travel. Once it's hitting those areas I expect it to be the #1 killer in the US.
Depends on the country and the age pyramid. IFR in Italy is 1% fir the flu as well as for C0VID-19, so just 1x, not 6x higher. For Germany I got to 2x.
Lung damage is of course a serious issue, yes. And ICU overload which does not happen with the normal flu.
These numbers seem much more realistic versus the previous doomsday predictions of 3%. To compare this to base rates, the age adjusted base rate for deaths in the US in 2018 was about 0.7%[0]. Depending on how you look at it, this is either really bad (i.e., 6x worse than the flu) or not that bad (i.e., less deadly than death by any cause).
3% would have been really bad, that's more than 3x higher than the normal death base rate.
The comparison is meaningless and maybe anti-productive. What you're saying harkens back to political fights about what are the numbers. The first sentence of the article is:
The overall death rate from covid-19 has been estimated at 0.66%, rising sharply to 7.8% in people aged over 80 and declining to 0.0016% in children aged 9 and under.1
Nearly 8% death rate for folks over 80 is pretty remarkable. If people out there start saying "it's just 0.7%! Less than the flu!" old people will not take the precautions they need to. Because of the contagiousness of this virus, it should be treated as the huge monster that it is by old folks.
There should be a rule that anyone publishing percentages is required to also publish the absolute number for their country. Based on comments I've read on social media, many people simply can't reason about percentages: they post about how the death rate is "only 1%" but are horrified when told that implies 2 million dead in the USA. One of those numbers seems very small to them while the other seems unbelievably large. They're the same!
The follow-on effects might even be worse than this.
Worldwide, people are living longer. If this virus is more problematic for older people, then they will take up all the medical resources. And they will continue to infect more health care workers.
The result, is that there are now less medical resources, to handle those that don’t have the virus, but have other medical issues. The medical system may collapse, and these people will die.
This is exactly the problem that hit Wuhan. Their medical system collapsed from the overload, that other people began dying. And those that didn’t have the virus, went to the same hospital to get help, and got the virus at the hospital. So now, they have both, their medical problem, and the virus.
Sadly, this appears to also be happening again, in New York City.
It will be years before we get proper studies, but there are also going to be deaths caused by the COVID-19 situation. I'm about to take my wife to a clinic because she sprained her ankle. All of the nearby clinics have been converted to handling COVID-19 cases only, so we have to go to one much farther away. Luckily a sprained ankle isn't typically life threatening, but if it was, driving that much farther could have led to a negative outcome.
No matter how much I hide at home and don’t do anything risky, I can’t help but worry about things like appendicitis. Something that most days would be dangerous but manageable if I catch it in time, would be much worse right now.
The reasons for it being so serious is not the death rate, but the rate of spread, due to lack of immunity, if you do nothing then hospital system gets overloaded and you will start seeing much higher death rates (see Italy, Spain) and not only from covid but across the board, heart disease, accidents people not receiving planned care and their chronic conditions worsening etc.
It's not just the hospital system and it's not just the deaths, terrible as they are.
You don't want a significant proportion of people in other key industries - policing, food production and distribution, utilities, logistics - off sick at the same time, because those systems will start to fail.
And in many countries people in those industries are being sent home if they show any symptoms - never mind serious symptoms that require hospitalisation - because some of those jobs are public-facing.
There's an obvious danger that a relatively small number of workers who deal with the public can infect a very large number of people.
This is similar to the best estimates we've had so far for the death rate with great care. Even then doubling the yearly deaths is still a very large event, and that's if we can flatten the curve enough that the health system copes. If not multiply the number by 5x.
At the cellular level it’s a numbers game. The more enemy combatants, the sicker you will be. The more exposure to the virus, the more viruses you’ll have in your body, the more intense the symptoms.
Hospitals don’t have great access to fresh flowing outside air. So as they fill up with infected people the air just becomes a cesspool of virus.
This is somewhat at odds with 21% of recorded outcomes so far having been deaths. There would have to be a hell of a lot of undiagnosed cases to bring that down to 0.66%.
Iceland tested their entire populace and found several people who tested positive but remained asymptotic while infected. Given that testing in most countries is limited to people who can get into their doctor’s office the people who get tested and who test positive have more severe symptoms. There are probably a lot of people who have it and are spreading it unawares.
I'm always sceptical with people said to be asymptomatic. It might be asymptomatic for 3-28+ days. The existence of antibodies will be a better measure.
There are also a couple of articles floating around that look at total deaths in certain regions. Unfortunately there's a lot of variability but e.g. in some areas in Italy, non-Covid-19 deaths are >4x what they were at similar times in the past, which suggests that many Covid-19-related deaths are not being identified.
Whatever the confusing data in this epidemic might say, there are unquestionably a hell of a lot of undiagnosed cases. 10x to 100x depending on your country's testing.
When I assume a reasonable lag time between a case and death, the figures I am seeing (worldometers and elsewhere) seem to be about 5%.
Then the difference between 5% and <1% would presumably be all the mild cases that aren't diagnosed.
If you look at the percentage of outcomes in the graph on worldometers' page, which I think you're getting ~20% from, it declined and then increased again; it is clearly not converging (yet) to the number people really want to know.
Edit: we've banned this account for breaking the site guidelines repeatedly. Please don't create accounts to do that with. If you don't want to be banned, you're welcome to email hn@ycombinator.com and give us reason to believe that you'll follow the rules in the future.
They quoted communist as if it were a quote from other comments in the thread... And plenty of "Democratic" countries such as North Korea have authoritarian regimes. It seems that without significant effort or intervention that governments can become authoritarian regardless of their purported underlying system of governance.
Flamebait like this is not allowed here. If you have substantive concerns about, say, data, it's fine to post about that thoughtfully. "Communist China subverting the West" is the opposite of that, though. Please don't toss bombshell rhetoric into HN threads, it just blows everything up into crap.
That's not the point. The point is, you're taking HN threads further into flamewars by posting unsubstantive comments with inflammatory rhetoric. We ban accounts that do that. No, that's not because we're communists. https://hn.algolia.com/?dateRange=all&page=0&prefix=true&que... It's because HN exists for curious conversation and you can't have both that and flamewar. So please stop.
China is communist. That's not exaggeration. That's not hyperbole. That's not based on bogus data. Etc.
If you want to fault the original post, please feel free. But to call stating the obvious flame-y is simply nonsense. It's head in the sand, history denying naivete.
Please don't fault me for the collective foolishness.
Let's agree that that's a fact. That alone does not make for a good HN comment. Indeed if you just use a fact like a club to bash opposing views with, you're doing damage regardless of how facty you're being.
There are infinitely many facts. They don't select themselves; people choose which facts to use and then choose what to do with them. Please don't do flamewar with them here.
You are one of already three commentators saying this (see https://news.ycombinator.com/item?id=22785738 and https://news.ycombinator.com/item?id=22785762), and similar concerns arise every time numbers from China are mentioned, so I think that there's no need to worry that you are advancing some controversial point of view. (For that matter, it's probably worth being equally suspicious of everyone's numbers, the US's probably in particular; but these are the numbers we have, and better to start work with flawed data than to ignore all data until we can gather perfect data retroactively.)
I'm a scientist, we have a saying in my field. Garbage in, garbage out. If the data from China are wrong, then including them in calculations will make all of your calculations worse. We know that China's numbers are not only suspect but actively manipulated, as such we should not be using their data for calculations full stop.
GIGO is a good principle to keep in mind, but nobody's numbers can be absolutely trusted here; every government has incentives, both from good motives and ill, to make things look as good as possible—and even when there is no conscious bias, various decisions will at least mean that numbers from different countries are probably not really comparable. Thus the normally scientifically sound principle of not allowing in suspect data is indistinguishable, in terms of its effect, from simply ignoring the available data. Better to regard the data as suspect, and do as much statistical analysis as possible to deal with it.
(I think, for example, of data gathered on the enemy during wartime, which are also constantly somewhere between unreliable and falsified; but we use them anyway, knowing that they cannot be completely trusted.)
As a scientist, it's also wise to question the data. Where it came from. If there was motive for that data bring falsified / manipulated, etc.
In the context of Communist China then it's unreasonable not to be suspect. And yes, the USA's data should be questioned as well. But the OP link was China.
The tone behind chiefalchemist's comment is not appropriate ("Communist China" intends to evoke specific emotions, which doesn't have a place on hackernews).
That said, while the citation for this is unlikely to be widely trusted, there is a kernel of truth here. Can't find a specific citation for the reason behind the underreporting, but the underreporting has been widely discussed, as has the misinformation campaign attempting to relocate the source outside Hubei.
In any case, I'd like to see more research that accounts for totals from only countries that are accurately reporting their data. Unfortunately, that might not be for a while until e.g. Iceland has a chance to give their numbers now that they're testing literally 1/8th of their population. As other comments have suggested, cruise ships could also be another good data source.
Looking forward to constructive discussion on whether or not numbers from countries such as China and Brazil can be trusted.
I’m no statistician, but I’m very doubtful of the numbers coming out of China. I’d be interested to see how this changes with any given countries data excluded. My suspicion is removing China’s would move the needle more than any other country.
I have seen many articles with similar thoughts - that the death rate of Covid is < 1%, similar or less than the flu and other well known viruses.
But, anecdotally, two close associates have died of Covid, and a neighbor is now on life support. May he get better soon!
I (fortunately) have not heard of anyone even being put into a life-threatening position by Flu. Asking a few friends, their experiences match mine, though the victims differ.
Can someone with more understanding explain - are we just the exceptions, or is there some reason that the anecdotal evidence is so far different from the numbers?
Every year about 295-650k die of respiratory issues with flu as a complication. That means on average a 30-year-old knows about 200 times the people who have died of the flu then Covid.
So you must certainly be an exception. Personally, I don't know anyone who knows anyone who's even been hospitalized.
Common flu does not have a ~1% CFR. More like 0.1%. So those articles are (deliberately?) wrong. If you mean "less than the 1918 flu", then yes you're right.
One more data point here, I too do not know of anyone who has died (or even been hospitalized) with influenza, despite my having a large social circle including plenty of elderly. I don't know of anyone who has died of covid yet, but our county has only had single digits confirmed cases yet. One of which is a well known farmer in the area, and he is hospitalized currently.
Again maybe just an anecdotal outlier but I know quite a few people that have died of the flu, from a couple kids when I was young to some of my elderly relatives.
{kind=link}
This uses a data source independent from what the paper uses. Here's the calculation...
Current Diamond Princess' CFR (Case Fatality Rate) is at 11 deaths / 712 infected = ~1.54%. Ten more are in serious/critical conditions, so it could increase.
Since testing in DP was almost universal, IFR ~= CFR.
DP's demographics is representative of > 30% of population of many/most countries. (See figure 1 here: https://wattsupwiththat.com/2020/03/16/diamond-princess-myst...)
Assuming no one in other age groups/health conditions in a country of interest dies (unrealistic) and everyone from Diamond Princess who is in severe/critical condition recovers (optimistic), population's IFR would be = 1.54%/0.3 = ~0.51%.
Also, cases from Diamond Princess have received good care. If the healthcare system gets overwhelmed as has happened in many places, population's IFR would shoot up to multiple times as high.
Thus, 0.5% is a lower bound for COVID19's IFR, unless a better treatment protocol/medication is invented. Alternatively, if there are successful measures to shield the elderly from getting infected, a region's overall IFR could be lowered.