This is revisionism. The only place in Europe that didn't lock down was Sweden and they were viciously attacked in the media for it, additionally Anders Tegnall was also attacked by other epidemiologists.
I followed it all very closely at the time. Tegnall and his mentor stood alone. With the exception of the Great Barrington crew and maybe Ioannidis, all the other so-called experts were loudly and vocally demanding lockdowns as a strategy. Great Barrington meanwhile was viciously attacked, described as fringe, non-consensus, would kill millions etc.
The attempts to rewrite what happened in this whole thread are incredible to witness (not just your post, many others). It was only a few years ago! Our memories aren't that bad! And the internet is full of receipts on this. The idea there was robust academic debate about lockdowns or masks or the lab leak or anything else is a fantasy.
> all the other so-called experts were loudly and vocally demanding lockdowns as a strategy
This is not true. Denmark, Finland, Netherlands and UK [1] had their own versions of "Tegnell". That is, epidemiologists who recommended the let-it-rip, "herd immunity" strategy. In these countries, politicians finally decided to follow the majority consensus among countries, and ignore those epidemiologists who were among the "herd immunity" school of thought.
Even in New Zealand it was a somewhat close call, would the government listen to Michael Baker [2] as they eventually did, or Simon Thornley [3].
> Great Barrington meanwhile was viciously attacked, described as fringe, non-consensus, would kill millions etc.
Maybe because it was somewhat fringe, definitely non-consensus, and would kill millions?
[1] "For a time, he advocated a herd immunity approach."
Vallance is in no way comparable to Tegnell. Valance and the other UK/SAGE "experts" were quite happy to invert their advice overnight on the basis of nothing. Like all the others they were making decisions based on politics and ideology, not a mature of understanding of science. Tegnell picked one position and stuck with it because there was no reason to change it, in that he was virtually alone.
> Maybe because it was somewhat fringe, definitely non-consensus, and would kill millions?
It's amazing how many people still never got the memo that lockdowns and masks had no effect whatsoever. This isn't even up for debate anymore, the data is openly available and has been analyzed to death. These interventions simply did not work, and it was known from the start that they wouldn't work. Heck the idea they wouldn't work was the consensus right before 2020, which is why a "consensus" of these idiots is worth less than the electrons used to transmit it.
It's amazing how many people still never got the memo that lockdowns and masks had no effect whatsoever.
Do you have a source for that? It's been a while since I've looked at Covid numbers, so the only research I know off the top of my head that claims there was no effect is a meta-analysis by some economists, which originally claimed lockdowns only prevented 0.2% of deaths. After criticism, they had to re-evaluate their approach and arrived at 3.2%. However, not all objections were addressed, so who knows if there isn't another order of magnitude hiding somewhere.
Personally, I've been leaning towards lockdowns having the potential to be effective based on excess mortality in the nordics: Sweden was the only nordic country that did not lock down in March 2020, and it's also the only one of these countries that saw significant excess mortality in April 2020. There could of course be another reason for that, but until someone offers such, the lockdowns seem to be the obvious factor...
Perhaps your April 2020 number is correct but I think it's irrelevant because it is too time-boxed. I did an analysis (matching those by others) using the OECD excess deaths data and if you extend the time period through last fall, Sweden did either best (according to other's analysis) or second best (according to mine). Excess deaths actually continued after the pandemic has subsided in many countries (US and UK at least I recall) and I think it reasonable to assume the pandemic and pandemic policy had something to do with it. To judge overall success of policies you need to look at the whole time of the pandemic and its aftermath and the Swedes did better than almost everyone
Due to large numbers of immigration, Sweden has younger population than comparable nearby countries. Too many excess death analyses just take the average of 5 previous years (2015-2019) as the baseline, to compare yearly or weekly deaths to. But in countries with ageing population, number of yearly deaths have been on a slowly increasing linear trend already for a long time. If you ignore the trend, and only compare to the 2015-2019 average, all countries with ageing population would show continuously increasing excess deaths.
Also, Sweden has a peculiar bookkeeping system, and a surprisingly large number of deaths are recorded without precisely known date. If you only look at weekly death statistics, you will miss the "week 99" deaths from the yearly total.
All valid things to check but would also need to be checked for other OECD countries. I would not assume the OECD methodology does not take account of the aging. Also I would not assume this had much of an effect. The way it might would be if a lot of younger people moved to Sweden during the pandemic . In general cross border movement slowed during that time
> I would not assume the OECD methodology does not take account of the aging.
And here you would assume very wrong.
OECD does indeed estimate excess mortality simply by comparing to the 2015-2019 averages:
"The expected number of deaths is based on the average number of deaths for the same week over recent years (in this case the previous five years, 2015-19). This baseline could be considered a lower estimate of the expected number of deaths since both population growth and an ageing population would be expected to push up the number of deaths observed each year."
"Importantly, given the impact of COVID-19 to the overall number of weekly deaths in 2020, the
average deaths for the period 2015-2019 continues to be used to calculate excess deaths in 2021,
and still applies as the base for 2022 and 2023 excess deaths."
From their: Methodology_All-cause-Excess-and-COVID-19-deaths_OECD.pdf
> Also I would not assume this had much of an effect.
Also here you are assuming somewhat wrong.
For Finland, the 2015–2019 average annual deaths is 53723. 2022 deaths were 63219. Thus the simple, OECD-style, estimate for excess mortality is 9496.
Whereas an age-structured model from Statistics Finland estimated 56158 deaths for 2022 from pre-covid trends. So the age-structure-aware excess mortality estimate is 7061 for 2022 for Finland.
Curious. At the time, I also made a pretty picture comparing deaths in 2020 to the 2015-2019 average (ignore the drop off at the end, as the data was incomplete at the time):
Early on Sweden had more deaths which led people to argue lockdowns worked, but then things subsided and other countries caught up and then surpassed it, leading to Sweden ending up near the bottom of the COVID death league tables (in Europe).
It's also important to remember in all this that the lockdown policy wasn't predicated on making a small difference you need powerful statistics to find. It was advertised as: anyone who doesn't lock down will experience mass deaths and full blown collapse. Epidemiologists claimed Sweden would experience double the usual death rate due to COVID, i.e. as many deaths from COVID as from all other causes combined! Their actual death rate:
There's a tiny bump in 2020, but at least part of that is simply noise due to 2019 having an unusually low death rate, so you'd expect it to be higher than normal in 2020 even without COVID.
Yes if you look exactly at the early pandemic then Sweden did worse than its immediate neighbors (but not worse than the rest of the OECD countries). But the real measure of success in policy has to include the rest of the pandemic and its aftermath. The others caught up.
But severity and timeline of lockdown measures varied from country to country, ie there was some diversity of opinion. Also note that even Sweden eventually implemented policies such as restricting opening hours of bars and restaurants, limiting the size of some gatherings, etc. for a time.
A scientific consensus is significantly different than media opinion.
Second, there is no "debate" regarding efficacy of masks and limiting exposure via quarantining. Masking reduces the likelihood of contracting SARS from others, and staying home reduces the spread to others and strain on hospitals. Unsurprisingly, the people attempting to debate this typically had no medical background whatsoever.
Millions died in the US alone, and a non-trivial percentage of them would likely still be alive if our public officials did a better job of respecting the medical professionals and their recommendations.
Oppositions to lockdowns were never about whether they would reduce deaths or not in the short term. Anyone with a brain could understand that if people weren't in a position to breath on each other, the virus wouldnt spread as quickly.
Oppositions to lockdowns were always about tradeoffs and whether they were worth it. Its just such a boring critique.
My main question still remains, what would your plan have been if we still didnt have a vaccine? From my perspective lockdown supporters got completely bailed out by one of the greatest medical/scientific achievements in human history (developing and deploying an extremely effective vaccine within 1 year).
The only thing lockdowns do is push cases into the future.
Pushing cases into the future was always the stated goal of lockdowns. That was what "flatten the curve" meant. The idea was to accept some temporary consequences in order to prevent deaths until vaccines could be made.
I also don't think it was any stroke of luck that resulted in vaccines being made quickly. Our scientific establishments correctly devoted their resources to developing vaccines. A lot of us were closely following their development and knew that they were just around the corner. Even without advancements in MRNA technology, other types of vaccines were being made that could prevent the majority of deaths.
> Pushing cases into the future was always the stated goal of lockdowns. That was what "flatten the curve" meant. The idea was to accept some temporary consequences in order to prevent deaths until vaccines could be made.
The idea we needed to "flatten the curve until a vaccine" was obsolete the day many states closed their completely unused field hospitals. That should have been the indicator that covid wasn't nearly as bad as predicted. That was the day everything should have gone back to complete normal.
These lockdown "experts" never had an end game. They kept pushing the goal posts further and further until they completely lost the plot. That was one of my first objections to such mitigations. There was zero success criteria. Fuckers were just winging it. Which might be okay for some minimally invasive crap like enhanced handwashing protocols but it is absolutely bat-shit insane for something as impacting as lockdowns.
What we did was insane. I still have no idea how people look back, given all the data, and say "yup, what we did made sense". None of it make a single ounce of sense at all...
When "flatten the curve" came out as a slogan they told us 2 weeks. Absolutely no one in public health believed that would be true. It doesnt make sense on any level whatsoever. i mean it just beggars belief that they told the public that with a straight face. the only person i recall in early days of 2020 saying this was going to be many months if not years was Mike Osterholm which i respect for not gaslighting the public.
heres an article in the NYT about managing vaccine expectations.
also you argument falls apart when lockdowns (restrictions, npis, whatever you want to call them) continued way beyond vaccine rollout. I was first in line to get vaccinated and im very glad i did, because they promised us that would be a return to normal, but it wasnt for at least a year afterwards and i still havent been given an explanation why.
I'm just guessing, but an obvious reason would be because the vaccines were not as effective against the new variants? As in, while the vaccines still protected the vaccinated person, they did not effectively prevent spread of the disease, so other ways to do so remained relevant...
About a year after vaccines became available, only 60% or so of folks had received two doses [0]. Public messaging from the initial administration is an obvious contributor to the remaining 40%.
County / MSA hospital capacities, percent available ICU beds, ventilator use, admission increase rates, deaths, and various other stats were factored into restrictive policy decisions. However, this varies city by city and state by state (I suppose as an effect of federalism).
im sorry, but people who chose not to get vaccinated knew what they were doing and governments and public health officials holding everyone else hostage cause some people wanted to engage in risky behavior is not justifiable under any ethical framework i can think of.
“im sorry, but people who chose not to [follow the speed limit] knew what they were doing and governments and public safety officials holding everyone else to a [speed limit] cause some people wanted to engage is risky behavior is not justifiable under any ethical framework i can think of.
no because this is a terrible analogy. Speeding endangers others who have not consented to that danger, not getting vaccinated has absolutely no societal risk in this particular scenario with covid.
If I could make my car crash proof (me getting vaccinated in this analogy), i would have no issues with people wanting to drive as fast as they like (they already do it anyway).
that was published in 2021 about data from march 2020 to nov 2020, its completely irrelevant. I mean can you at least try?
also, even if vaccines did stop transmission your argument still doesnt make sense. I can protect myself by being vaccinated. I dont give a shit if the person next to me is unvaccinated, im already protected myself. If you decide not to, you are consenting to increased risk.
Who would win - a peer reviewed article from the New England Journal of Medicine with published methodologies and citations? Or some internet rando with no medical background simply saying “that’s irrelevant”?
Also, you’re misreading the article; please review.
> Oppositions to lockdowns were always about tradeoffs and whether they were worth it. Its just such a boring critique.
Fully agreed; saving lives / community responsibility is the noble choice. Unfortunately, many folks in states with poor education (e.g., Texas), would make remarks questioning the actual existence of the virus - even after Trump contracted it and was treated at Walter Reed.
But, work on a vaccine began almost immediately, no? I trusted that shifting the focused lens of US policy toward medical research would produce some incredible results, especially with the private sector pharmaceutical behemoths battling it out, so to speak.
yes "started." there was literally no guarantee we would even have a vaccine at all. There was absolutely no historical precedent for development and deployment of a vaccine with a year of virus discovery. it was incredible achievement and government official literally bet the entire world economy on it for some reason i still cant understand.
> Anyone with a brain could understand that if people weren't in a position to breath on each other, the virus wouldnt spread as quickly.
This can be rephrased as "it's just obvious/common sense that lockdowns work" and it's a really common argument, but wrong.
Unfortunately there's nothing really obvious or intuitive about viruses. The Diamond Princess cruise ship showed right at the start that lockdowns would be ineffective. They locked down everyone on the cruise ship the moment the first outbreaks were confirmed, confining them to cabins. In the transmission model that lockdowns rely on that would have ended the outbreak immediately. But it didn't, instead people kept coming down with COVID completely at random, scattered all over the ship. From this two things could be concluded:
1. SARS-CoV-2 is airborne, that is, it can move long distances in gaseous clouds, i.e. through air ducts, by hanging in the air for long periods and other ways that lockdowns can't affect.
2. The clouds must have circulated through the ship, yet not everyone was susceptible.
This wasn't a terribly surprising result because investigators had concluded the same things about SARS-1 back in the day. SARS-1 clouds were able to move within apartment buildings even when everyone was locked down in their apartments, apparently via air ducts.
Some people pointed out at the time that this would render lockdowns irrelevant right back in March 2020, and were ignored, but time has proven them right. There's no correlation between lockdown severity and results.
I have a medical background and when the pandemic started I did a literature to see if masks had helped with other respiratory virus epidemics (as masking had been common for years in many Asian countries ). the results were decidedly unimpressive and I concluded masks might to something but it was not a big effect at a societal level. The mistake that many smart people without medical backgrounds make is assuming that if a measure "makes sense" from a basic science point of view, it must have a real effect in a patient or a society. Counter-intuitively this almost always turns out to be wrong.
I did a study of mask based on self reports early in the pandemic and I did show a significant slowing of the progress of the pandemic in states that had a high claimed rate of mask use. I had (I thought) some clever ways of eliminating other differences between states in my analysis and was surprised to see so much slowing. However, I am not sure which way the causality runs. I can easily see heavy masking making it such a bummer to go to bars (e.g.) that the lack of socialization caused the slowing.
But in summary, to your point, to the medically knowledgeable there was a lot of evidence before that masks would not do much (not nothing) and there is a lot more now that masks didn't do much
Please share your background so we can more accurately asses your credibility; saying that masks are ineffective is, at this point, painfully ignorant.
The nurses who thought so are either fired, dead, or updated their thinking.
No, saying masks work is the ignorant position here. There is no robust evidence that community masking has any effect, and people have looked hard for it. You can easily confirm this yourself because mask mandates had no impact whatsoever on case growth as can be seen by literally anyone who looks at the public test results data.
But if you don't trust your own eyes, maybe the Cochrane Collaboration is enough for you? They published a meta-review of mask studies.
Remember, you don't get to claim you're right because you fired everyone who pointed out you're wrong. It's painful to accept this, but masking was a lie from start to finish which is why the position of all the medical staff at the start was that masks don't seem to do anything and there's no evidence community masking would help. That position was correct. They changed it later for ideological reasons and the politician's fallacy.
These data showed statistically significant lower averages of SARS-CoV-2 daily infection in counties that passed mask mandates when compared with counties that did not.
The difference-in-difference analysis revealed a 16.9% reduction in predicted COVID-19 cases at the end of 30 days.
You might want to look into why meta reviews, particularly those plucked from popular COVID forums, aren't the bees knees you seem to think they are.
That paper isn't robust evidence, it's the kind of joke quality that typifies masks-work papers actually. RCTs are how you try to decide whether a medical intervention works, they're considered the gold standard for a reason.
Problems with this paper:
1. It's just a study of public data so should be trivially replicable, but they picked data points "via Microsoft Excel’s random number generator function" so it's non-replicable by design. Right up front this makes it incompetent work because there'd be no way to detect P-hacking.
2. Because it's not an RCT they can only show a correlation, not a causation, yet their claims are causal. An obvious confounder is that going out with a mask is no fun so you'd expect people to socialize more in places without a mandate, yet this isn't mentioned.
3. The effect size is tiny: ~4 cases a day! In counties with tens of thousands of people! This is NOT how mask mandates were advertised to the population.
4. "We did not record compliance with mask mandates". Yes I'm sure the residents of places like Anderson County Tennessee followed public health orders meticulously.
5. They ignore all the contradictory evidence.
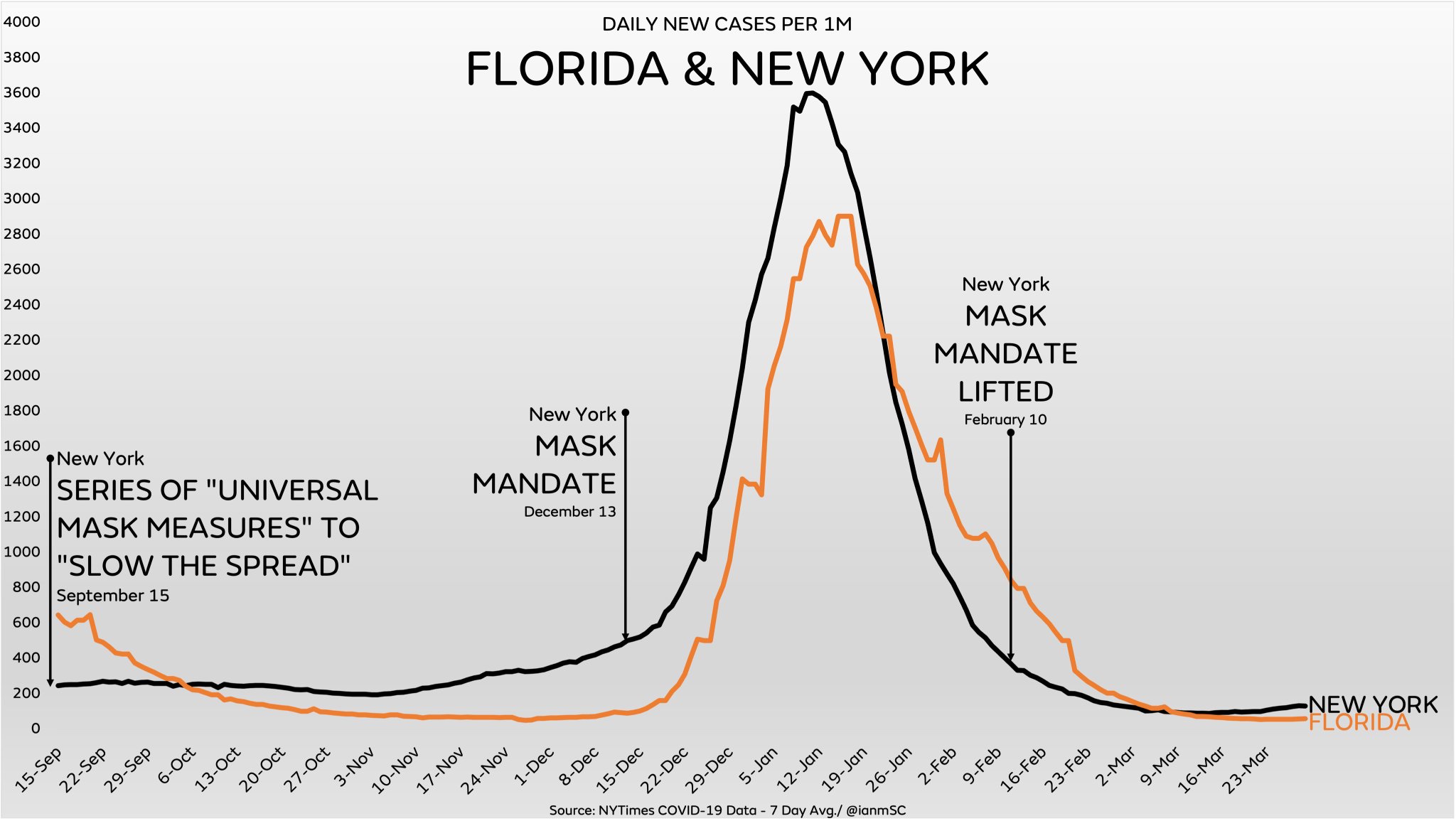
Again, I cannot stress this enough, we know mask mandates don't work because of the times they were introduced with no change in case trends. Here's a single example:
Because the claim is "mask mandates always reduce transmission", it only takes one counter-example to disprove the claim. There are hundreds of charts like that one, but only one is required. That's the nature of falsifiability.
To conclude that mask mandates work you have to be able to explain the times when they didn't. Crap studies like this one (cited 3 times, well done for finding it) are produced by academia all the time, but they get ignored because they can't explain that, and the authors are invariably biased. These guys even cite a claimed 0.5% reduction in cases and call this "effective"! Imagine if governments had stated up front when imposing mask mandates for the first time, "we think this will be effective because it might reduce case counts by half a percent". What would people have thought of the sanity of this cost/benefit tradeoff, exactly?
> Unsurprisingly, the people attempting to debate this typically had no medical background whatsoever.
You don't need to have a "medical background" to debate lockdowns or masks. The decision to use those should never have been made exclusively by people with "medical backgrounds". It isn't their job. Just because the "medical people" say it's gonna work, doesn't mean it is worth the cost to society. And it isn't at all the place of people with "medical backgrounds" to figure out what those costs are and if they are worth it...
"Experts" shouldn't be decision-makers. They should only inform decision-makers. A good decision-maker should take input from everybody who will be impacted. This was never done at all. Had it been done openenly and transparently we'd never have done lockdowns, school closures or anything else. Such things are completely insane no matter how much "medical experts" suggest to use them.
> A good decision-maker should take input from everybody who will be impacted.
You’re right; I’m really glad I polled thousands of fellow employees before forcing multifactor auth, or that time I chatted with a sysadmin to make sure they really did mean to open RDP on a public server before taking it offline.
Sarcasm aside, in a time of a medical emergency, it is the job of medical professionals to make decisions, because public safety supersedes individual freedoms. It’s why we have speed limits. It’s why you have to wear a seatbelt. It’s why you can’t shoot fireworks off during a drought. It’s why products are restricted from being sold. The concept is fundamentally the same.
It’s also the same reason I’m glad cybersecurity policy, strategy, and operations are not a truly democratic process.
> Sarcasm aside, in a time of a medical emergency, it is the job of medical professionals to make decisions, because public safety supersedes individual freedoms.
This might be true for like the first week or two of march but after that... the response should absolutely not be solely in the hands of nothing but "medical experts". Those people were never elected, are not accountable at all for their actions, and were granted virtually unlimited control. That is what we call a dictatorship.
I would much, much rather have a diverse party of people calling the shots and not just one very specific niche class of "expert". Without a diverse set of people involved you'll wind up where we got... an extremely myopic fixation on exactly one single respiratory virus for two+ years to the complete disregard for the damage it caused to our children and communities.
I used to think technocracy would be awesome. What better than to have a bunch of experts doing things "the right way". But covid opened my eyes to how incredibly bad of an idea that is. Experts are only expert on one specific thing. All their advice and mandates are made through that narrow lens.
> You’re right; I’m really glad I polled thousands of fellow employees before forcing multifactor auth, or that time I chatted with a sysadmin to make sure they really did mean to open RDP on a public server before taking it offline.
But you also chatted with business people to get insight into the costs of forcing multifactor auth on people would be worth the security gains? Right? Because forcing 2FA is absolutely not something a security expert gets to decide. A good security expert would realize they are an advisor and not the person calling the shots. They know their role is to outline "what would happen if we did blah blah" and then let the business people know the pros and cons so said business people can make a decision. The business people, if they are any good, realize that there are multiple often conflicting requirements and have the hard work of deciding what the right tradeoffs to make are. Experts don't get to decide those tradeoffs at all...
I mean, could you imagine if the only input you got for a product, say a car seat, was just from a bunch of lawyers? The product would be absolutely lawsuit proof but I bet it would suck as a car seat.
> the response should absolutely not be solely in the hands of nothing but "medical experts"
This wasn't the case, and to say so is a blatant misrepresentation of the past. Did Fauci issue a travel ban, enact the Defense Production Act, or redirect the supply of medical equipment? Did the CDC somehow supersede congressional authority and directly fund research via the CARES Act? Were appellate courts no longer hearing cases regarding COVID and civil liberties?
> you also chatted with business people to get insight [...]
this reinforces my point: anyone who happens to be impacted is not entitled to input. Conversations between medical professionals and public officials were occurring every single day. But - do you think Trump was genuinely listening to his advisors?
> there are multiple often conflicting requirements and have the hard work of deciding what the right tradeoffs to make are
that's exactly my point, again. No one knew it was going to mutate that quickly and stay an issue. The tradeoff for doing less was more people dying.
{kind=link}
{kind=link}
I followed it all very closely at the time. Tegnall and his mentor stood alone. With the exception of the Great Barrington crew and maybe Ioannidis, all the other so-called experts were loudly and vocally demanding lockdowns as a strategy. Great Barrington meanwhile was viciously attacked, described as fringe, non-consensus, would kill millions etc.
The attempts to rewrite what happened in this whole thread are incredible to witness (not just your post, many others). It was only a few years ago! Our memories aren't that bad! And the internet is full of receipts on this. The idea there was robust academic debate about lockdowns or masks or the lab leak or anything else is a fantasy.