I don't know why we're so hesitant to just close bars and restaurants everywhere, pay the staff generously, and leave the rest of the economy open. At least in the UK I think it would have stopped us from having a second lockdown.
Interesting thought. How much would that cost? And is it only restaurant direct staff that is compensated or also other industries that are negatively impacted by their closure?
There's an inherent tension, on the one hand, we cant afford to pay the wages of a 100 billion pound a year industry out of tax revenue. On the other hand we completely fucked up any of the potential ways we could have avoided doing that.
Well, sure they get paid, but what about the people who are deemed essential and still have to work? Seems kind of unfair to those people doesn't it? It's not an easy problem to solve...
Yes. The money isn't coming from my pocket our yours. It comes from a Central Bank punching keys --literally in the case of America's Federal Reserve-- on a keyboard and updating a ledger balance.
This is a terrifying and yet all too common view. When the central bank punches keys and creates money out of thin air this DOES come from your pocket and mine, but in a way that is not entirely as obvious as the way other costs are. It reduces the value of what was already in our pocket via inflation. The money in our pocket can no longer buy the same amount. That’s a cost.
God I wish we would go back to the gold standard so that the cost of government expenditures would be more obvious to the general public via payment from increased taxes or from allocation away from some other government expense. Instead, people are left thinking the government could magically solve all of our problems by printing more money, but for some reason doesn’t because it doesn’t care.
What inflation? Gold bugs have been telling me that inflation was going to happen for my entire 20 year adult life. And being on the Gold standard did not in any way prevent inflation...but don't let that little fact get in the way of your hard money talking points.
If you want to have an honest discussion about the inflationary effects of adding more dollars to the money supply, then we have to talk about where those dollars come from and why they do and don't create inflation. Talk about what the real demonstrable alternatives are, and whether or not a higher inflation is really the devil that so many claim it is.
Where’s inflation? See real estate, all financial assets, medical costs, and education to name a few obvious examples. For many of the items actually included in CPI numbers, the inflation has been outsourced to third world countries.
The real demonstrable alternatives are those we had prior to eliminating the gold standard. We are now able to print our way out of recessions, at the cost of an incredibly destabilized economy comprised of asset valuations that are so high they lead to perfect correlation downward when there is a shock to confidence.
Real estate is local, my house in Alabama has returned sub 1% annualized in appreciation, my house in Washington as returned about 6% annualized. Where supply is constrained, prices are going up, where there is excess, prices aren't even keeping up with inflation. Seems like a perfectly rational market to me.
Financial assets is far too broad a category, but "markets can remain irrational far longer than you can remain solvent" isn't some new statement. I'd argue that this is more a consequence of a confluence of factors including the end of general scarcity of capital, low interest rates, and low taxes.
Medical and Education costs are structural issues within the US, see most of Europe for a counter example.
As far as outsourcing, well that has lifted over 1 billion people out of poverty...so yea, I got nothing for you if you think American's being able to buy more goods for fewer dollars while simultaneously making the world a better place is something to be concerned about.
And our economy is far more stable today then any time in the history of the US. Or are we going to pretend that multiple depressions didn't happen in the late 19th and early 20th centuries? The only reason that the 2008 recession was as bad as it was, was because of a lack of political will to spend money.
Inflation hasn't become a reality since the other nations still trust the value of the US dollars as reserve. With so high trade deficits, we are essentially saying to the world, "sell me goods in exchange for the paper that I printed some big numbers on it", without getting as much in return.
Do you think this is sustainable in the long run? Will they keep giving us more goods/services than they get? What would happen if they decide to not use US dollar as reserve or they start demanding another currency for trade?
If the US dollar ceases to be the world's de facto currency, we have much larger problems then the moderate inflation that may or may not follow. I'd argue it is far more a political problem than a monetary problem at that point.
It’s “all too common” because it’s how most 1st world economies work (though to be fair: your fear-based view and false belief that it is anomalous is the true “all too common” viewpoint). Case in point is the US that has been running deficit budgets for decades - and yet it still exists! It is still an economic power house! The general disconnect is that nearly all discretionary spending is directed towards the military, which somehow eludes all those who ask the question “but how are we going to pay for that?” whenever anyone proposes providing money to people who definitively need it.
I am unclear on your first sentence and bracketed section. My point was that people generally share the view that printing money is without cost and that this is incorrect. The government cannot magically print money and provide goods and services without cost, via future tax increases or inflation. There’s no free lunch.
The cost is so low as to be non-existent. The downsides of printing money are effectively nil. If this were not true the modern global economy would have died out decades ago, when printing money became the primary method of commerce. Your concern here cannot rationally be a concern for printing money, a ship that sailed long ago. So I’d have to assume your concern is how the printed money should or should not be used. And in this case you were replying with concern to a post that recommended using printed money to pay high-risk people a sustainable income when their jobs should be furloughed. But instead of making a case as to why high-risk people should continue to sustain high-risk, you instead want to falsely claim printing money is significantly detrimental.
Central banks create money, but governments don't spend that money. They spend money from taxes and bond sales.
About $15T USD exist [0]. $5T are held by foreign banks [1], because the USD is the world's reserve currency. All of those countries want the USD to remain stable, so their own economies can work smoothly. The countries cooperate with USA and side with USA in disputes. This benefits USA greatly. If USA went to the gold standard, this benefit would disappear.
Currencies on a gold standard experience inflation and deflation due to changes in the value of gold. The value of gold is primarily driven by demand for jewelry and manufactured products [2]. Demand fluctuates with the business cycle. Gold value is also affected by supply fluctuations. On a gold standard, these would become extra unwanted currency fluctuations.
Only $9T of gold exists above ground in the world. USA has only 3,000 tons of gold, worth 3,000 t * (1,000,000 g / t) * (oz t / 31.1 g) * (USD$1840 / oz t) = $177B. So to get $15T of gold, USA would need to mine or purchase 250,000 t of gold. This is equivalent to 72 years of the world's current gold production. So to make it possible, gold production would need to increase dramatically. And it would take a while. Meanwhile, the US economy keeps growing, increasing the need for currency.
Gold mining produces huge amounts of crushed ore which continually leaches heavy metal pollution into the environment. Gold mining uses cyanide which occasionally leaks and sterilizes a river or lake and kills all the birds and other wildlife nearby. Increasing gold mining would increase suffering around the world.
Another option is to increase the price of gold. This would negatively affect industry, especially electronics manufacturing. It would also cause an enormous wealth transfer to India and other countries that hold a lot of gold jewelry.
On a gold standard, governments have limited ability to solve problems in money supply, and their currency is subject to business cycle fluctuations and interference from cartels. USA will have difficulty getting enough gold to back its currency. Increased mining will poison people in many communities and devastate parts of nature.
Some work still needs to get done. Society won't work if everyone sits on their bum for a year, pandemic or not. Among the jobs which need to be done, however, there are no restaurant workers.
For the same reason that a tourniquet is not a long-term solution to a severed artery. It is a short-term solution to a specific problem and it has a shelf life.
Surely by being forced to do lockdowns later on we are paying dearly for letting them stay open.
I think we can also have more fine-grained policies. In Scotland they simply disallow serving of alcohol in restaurants and pubs, and restaurants have to close by 6PM. Unsurprisingly Scotland seems to be doing somewhat better than England and has avoided a second nationwide lockdown.
The basic idea is if we can target the 5% of the economy that is causing most of the spread, you can keep the other 95% open.
> "I don't know why we're so hesitant to just close bars and restaurants everywhere..."
because despite the fearful hype, there's no evidence restaurants are significant sources of spread. bars, at least, are more plausible (because of social dynamics, not fluid or viral ones), but still not conclusively proven to be significant transmission localities. transmission is primarily happening in private social gatherings, not in public places like restaurants, gyms, or grocery stores where we see so much attention being misdirected.
this paper, like similar others, paints a possible but unlikely picture of how a couple infection cases might be related, out of probably thousands (millions? billions?) of other possibilities. it's a classic case of availability bias--creating an explanation based on the limited observed information at our disposal, while expressly ignoring the much vaster array of information we don't, or can't, observe.
it's clues tied together to create a pat narrative, not conclusive, nor even particularly persuasive, proof on how transmission happened in this scenario. it's only one possibility among many.
I'm not familiar with the research on transmission occurring primarily in private social gatherings. In fact, I've seen some researchers suggest the opposite. Do you happen to have any helpful links or search pointers?
no good pointers offhand, but the likeliest source is contact tracing programs. they understandably seem to be more focused on tracing over paper-writing. in any case, here's one published study from hunan: https://science.sciencemag.org/content/early/2020/11/23/scie...
this quote sums up their findings:
> "The average risk of transmission scales positively with the closeness of social interactions: the average per-contact risk is lowest for community exposures (including contacts in the public transportation system and at food and entertainment venues), intermediate for social and extended family contacts, and highest in the household. The average transmission risk in the household is further elevated when intense physical distancing is enforced, and for contacts that last longer."
the intuition is also pretty straightforward--we let our guard around those closest to us, who also happen to be those we spend the most time with. those are the two primary factors (closeness and contact time) for transmission. social gatherings are that layer just beyond the household where we are most exposed on those dimensions.
The way this is presented is going to be interpreted incorrectly. It is incorrect to compare percentages or probabilities like this.
Here is a different example to try and illustrate the problem:
Is 10% larger than 5%?
It is not possible to answer this question if the basis on which the percentages are calculated are different.
What if I said the 10% was 10% of whatever you last spent money on, but the 5% was 5% of Google's annual revenue. Which is larger?
The same thing is happening in the above - it isn't okay to calculate the probabilities in two situations and then try to cross compare them for size.
Sadly this error seems to be cropping up quite a lot! Matt Parker (Stand-up Maths) has an example of this and related to a recent election: https://www.youtube.com/watch?v=aokNwKx7gM8. His explanation is likely better than mine.
> How is this possible? Distancing _elevates_ within-household risk?
One obvious mechanism: Enforced distancing makes it less likely you get COVID from a source outside of the household, which (since infection usually provides some period of immunity) thereby increases the risk you get it in the household, on average.
This is also misleading. The paper does not intend to mean that "lockdowns will cause you to get infected by the people you live with". Which is what you seem to have written.
Restrictive measures do not increase your absolute risk at home. The paper was talking about the relative risk between two scenarios - which allows for misunderstandings. The last sentence which was omitted in your quote was:
"These lines of evidence support that SARS-CoV-2 transmission is facilitated by close proximity, confined environment, and high frequency of contacts."
What the paper ought to have said was, when more restrictive measures are in place, it then becomes important to focus and step up measures for the people you interact with most - because those people in this new and different scenario now become the most likely people for which you will catch an infection.
The people you interact with have not suddenly become more risky in an absolute sense, but they become a more important risk factor when situations change.
Trying to draw conclusions between the relative risks between two different scenarios is not the same as absolute risk. This is the trap!
no, it's really the government pushing infections to the periphery, so that it gets credit for visible action rather than meaningful effect (i.e., lowering death rates permanently without throwing half the population into severe distress). that's exactly the empty effort we should hold against politicians, especially when so much harm has blindly been brought to bear along with it.
it's unrealistic to expect families to social distance from each other for months on end for a pandemic of this severity (~0.5% fatality rate heavily skewed to the aged, as opposed to the 1918 flu with ~10-20% fatality rate across the age spectrum).
so the most impactful, and realistic, action to materially lower infection/death rates is to alter our behaviors around private social gatherings only (distance or mask indoors). focusing our efforts there would be spending our collective goodwill budget wisely, as opposed to the pointless political theater around masks and restaurants. instead, all of the focus has been on curtailing public settings (easier for the government to control), where only a small minority of transmission is happening (moreover, public behaviors changed without needing government intervention). it'd be farcical if it weren't so tragic.
no, the only policy we needed is to either distance or wear masks when visiting in private with those outside your household, not at home with family (which no one would do) or in most public settings (which are already very low risk because exposure in space and time is vanishingly low). that would focus our attention and effort on the most impactful situations, not the ineffective shotgun approach we have now.
This is an incredible writeup and hard to summarize (compress) since there is so much good stuff in there. Give it a read and don't forget to subscribe to Zeynep's substack. I rarely find that reading her is not either educational or thought provoking. Her writing also is non-polarizing and has a refreshing quality to it.
There's a number of sources on pandemic research that I consider authoritative, but none I've come to trust to the degree that I do Zeynep Tufekci. She's been the most rational, thoughtful, and proven voice on this since the beginning, and I consider her compiling, editing, and meta-analysis to be the gold standard.
note that they only evaluated the airplane itself, not the airport or transportation to the airport. "Being in a crowded airport or taking a taxi to get there could be a bigger concern, though."
I'm still not flying no matter how safe I am once I am seated on the plane.
On a strongly related note, are there any studies on outdoor transmission that are highly credible?
I've long assumed that indoor dining is likely a transmission vector, but since LA recently banned outdoor dining, I'm curious about any studies on that.
What I've been told is that LA did this with little scientific justification, and that outdoor transmission is rare. However, wondering what people on here more knowledgeable on the subject have found as far as peer reviewed research.
The problem with "outdoor" dining was all the tents restaurants were setting up in fall/winter. And it's exactly as you imagine it, no airflow or sun exposure with the vinyl / canvas / plastic walls and roofs.
> The problem with "outdoor" dining was all the tents restaurants were setting up in fall/winter.
But not in LA, which was what the GP was asking about. LA's climate is fine for regular outdoor dining all year.
> no airflow
From the paper this thread is discussing, it appears that no airflow is actually lower risk; the higher risk is having directed airflow, from indoor ventilation systems, and being in the path of that airflow from an infected person (and also facing them).
Anecdotally, we've walking a few OC beach towns the last couple weeks.. its _all_ vinyl sided tents everywhere outside. They're keeping in the heat for evening dining.
Afternoon dining is pretty easy to do, but dinner seems to be problematic even in OC where I'm at.
Interesting thing to me is recirculated air vs. contained air.
The vinyl sided tents aren't going to have recirculated air like indoors, but yes, the air is certainly not going to be flowing the way it would with no vinyl walls.
OC beach towns are as nice as they are unaffordable, lol. I love the restaurants there, though.
> Interesting thing to me is recirculated air vs. contained air.
The paper that started this thread notes that the only people who got infected in the indoor restaurant scenario they studied were the ones in the airflow path. Nobody else did, even though they were all in the same room with the same contained air. So this one study, at least, seems to indicate that just having contained air is lower risk; it's being in the airflow path of recirculated air that is higher risk.
That said, there is nothing in the paper that says that having uncontained air outdoors is not even lower risk than contained (but not recirculated) air.
We have a couple places in Portland that setup individual dining tents for just one table. Those were included in the shutdown of indoor dining, even though it seems to me that could be done fairly safely. It's a shame for those restaurants that put the time and money in to do everything possible and they still have to shut down.
Not sure if there are studies of that or not, but clearly a lot of these decisions are not "science based". Politicians are just taking the easiest path to optimize for a single metric, reduced spread, and ignoring all other concerns.
I love this. I think we dismiss "small data" too quickly. I see this all the time here on HN and in other places, where someone's experience will be dismissed as "just anecdotes", as if an anecdote contains no useful information at all. Statistical summaries by definition lose information--it can be incredibly valuable to continuously ask ourselves over time "What information is important to retain in our models/statistics, and what information is okay to discard?" To me, it seems obvious when I say it--well duh that's the scientific method--but it's so easy to become attached to our models and statistics and use those to dismiss important information as noise.
Well, it seems to me that it's not so much the size of the data that really matters -- it's whether the amount of data and the method of collection is appropriate to the question at hand. Certain questions only require small samples to answer. If you frame your null hypothesis as "the virus is aerosol therefore everyone in an indoor space has equal probability of being infected after a period of time", then a few counterexamples is all that is necessary to reject the hypothesis.
In the classic black swan example "all swans are white", it only took 1 counterexample (small data) to disprove the premise, while mountains of examples of white swans (big data) would be insufficient evidence to actually prove it. There's an asymmetry here.
Coming back to the article, the author recognized this exact asymmetry in the question at hand: "While some of this may look discouraging, I find these “small data” studies greatly empowering. They don’t just tell us what happened, they tell us what didn’t happen." "These small studies cannot tell us the proportion of transmission that occurs indoors, but they highlight how it occurs: droplets and aerosols being carried through the air. Clearly, the closer you are to the person, the more likely you are to get hit But equally clearly, air flow and the positioning of people are huge variables, too. Just talking doesn’t seem to generate aerosols to the point that everyone within the room is infected (though this is possible), but singing does—at least in these well-studied cases. Sometimes, though, the most important information is that the dog did not bark."
However, not all questions have this property. Let's say your hypothesis was something like "this vaccine will work in at least 95% of the population", small data approaches might not work. Bob and Jill said it worked for them -- how comfortable would we be extrapolating this anecdotal evidence to the general population? At most we can say there's a statistical signal to the affirmative, but nothing more than that. And that is the nature of self-reported anecdotal evidence (unless they were rigorously structured to remove confounding factors -- usually they are not).
p.s. Furthermore, not all questions require rigor, therefore anecdotal evidence can sometimes be useful without being rigorous. For instance I've always found Myers Briggs to be a "useful" heuristic despite not having any rigorous basis.
John Snow was able to disprove the miasma theory with "small data" (via analysis of people using a public water pump). This is how the germ theory of disease came about and helped save countless lives from cholera.
This is also how the science of (modern) epidemiology began.
You have to think of it like cigarette smoke. Aerosolized virus particles linger, and fill a room. If someone is close enough to you that you would smell them smoking a cigarette, they are close enough to infect you. It's why "social distancing" is just meaningless safety theater in an indoors setting.
That’s really not at all what these studies show. It’s direct airflow, over short periods of time. Your smoke theory would have everyone in both restaurants infected, which is not what happened.
I think it's a close enough analog. If there is sufficient ventilation, you might not smell it in one area but very strongly in another. If you place an infectious person in place of the smoker, you can guess where the danger zone is (not in the area free of smell).
You're right, of course, that cigarette smoke carries further and many more people will be able to smell it than there are people at risk of infection in the same situation.
>Your smoke theory would have everyone in both restaurants infected, which is not what happened.
Not everyone who's exposed gets infected, and most of those who do remain entirely asymptomatic. But some die. That's why this thing is so dangerous to the population as a whole.
There's endless amounts of computational fluid dynamics research being done on this. It's pretty clear that the virus particles are suspended in the air like smoke [0].
I find it amusing that there are just two mentions of COVID-19 in the small quote in the middle of article. Yet everyone completely understands what this article is about. Wondering how soon it won't be so obvious (probably not very soon, but still).
The whole opening bars/restaurants/casinos but closing gyms is mind boggling.
I understand keeping the population subdued with circuses, but you'd think politicians would realize the gym is a positive outlet that will reduce coronavirus deaths by having a healthy population.
My gym group broke up and 1 guy became overweight. Went from a no risk Coronavirus to high risk because Politicians messed up his routine.
Gyms are where there is the most aggressive breathing and grunting though, and that volatalizes as much contagion as people singing. Restaurants are a calmer more subdued breathing environment.
Yes, over the 332 days of 2020 on that chart, there are fewer deaths than the 365 days of 2019.
257 average deaths per day in 2020 vs 252 in 2018, which was the previous record high, putting 2020 on pace to become the new high record. That assumes that deaths are evenly distributed throughout the year, which at least in the US, they are not.
An annual snapshot of "excess deaths" lead to bad intuition. A weekly snapshot is much more helpful, leads to more accurate intuition, and generally is preferred.
The second chart is from October, based on the URL, and therefore missed the large spike of deaths in November.
Weekly snapshots are too volatile. If everyone who was going to die in March dies in the first week of March, but none die in the remaining three weeks, this will show a death spike whilst the number of monthly deaths is unchanged. If someone at the end of their natural lifespan dies a few weeks earlier or later than usual, this is not a national concern.
2019 was a weak flu season.
We need to examine this data across broader time scales to avoid the hysteria we are currently experiencing.
“But... what about countries such as the US and Brazil, where far more people have died of COVID than of any recent influenza? Less than 10,000 Brazilians die of the flu each year compared to 180,000 covid deaths.”
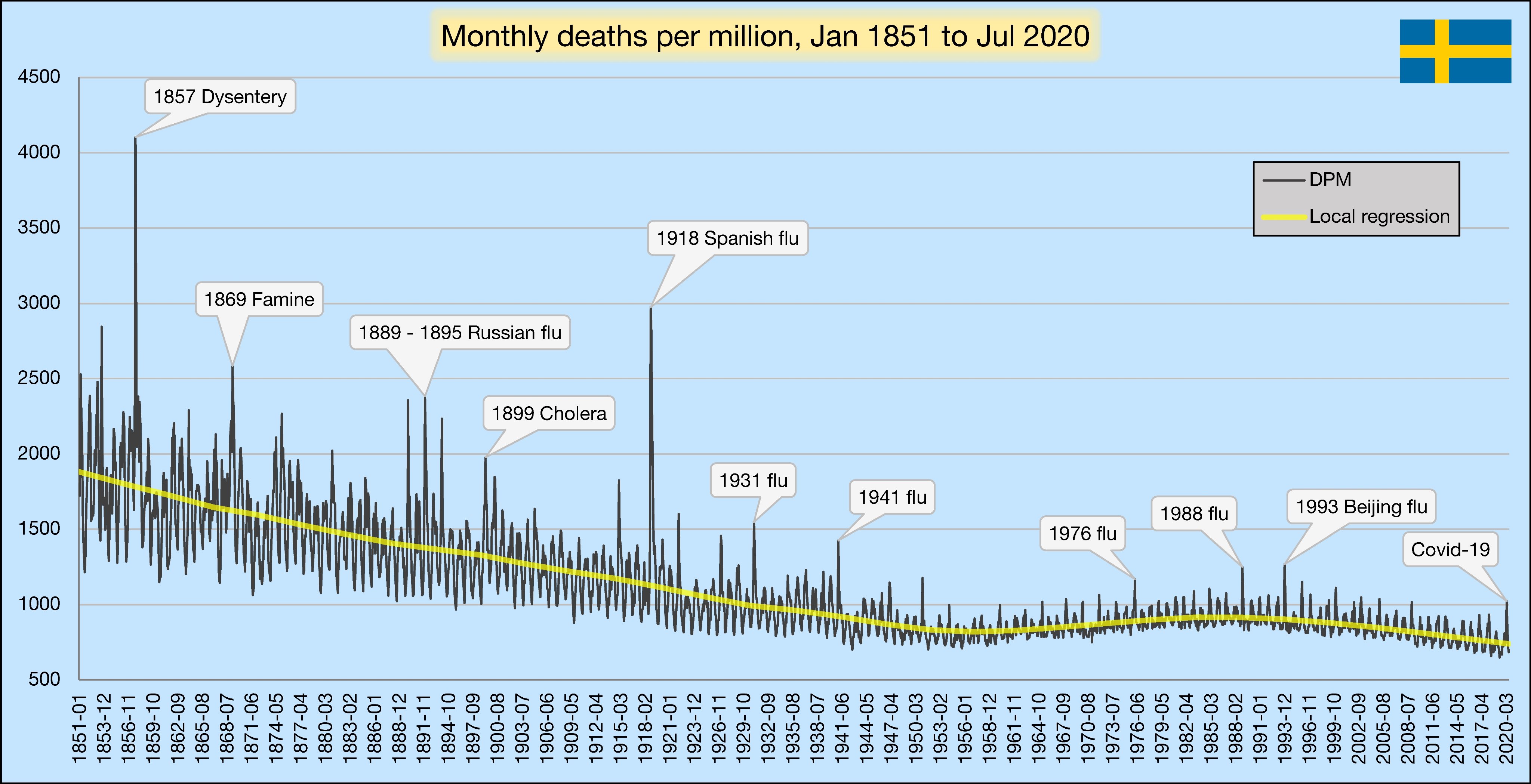
Everybody believes there are no restrictions at all and people carry on with their lives just like did before. Nobody talks about group gathering limits (smaller size than in most countries), that restaurants service hot food with much better safety than here in the States, etc. People still believe that Sweden's strategy is herd immunity without any interventions!
Presumably both people in this noted illustration also touched the door handle, possibly the door itself, and any number of other surfaces while entering the building?
I feel like drawing the link exclusively to air flow is tenuous at best. Saying with any level certainty that they didn't contract it _elsewhere_ seems dishonest.
* Only the visitors (cases A and C) sitting in the air flow path of case B were infected with COVID-19, while other visitors (V2, V3) closer to the infector for a longer period of time but in the absence of direct air flow did not become infected. In addition, the visitors sitting at tables with cases A and C (V1, V6, and V7) were not infected with COVID-19 because they faced away from the infector’s face. These findings strongly suggest that this outbreak occurred by droplet transmission exceeding a 2 m distance and excluded contact and fomite transmission. This transmission pattern is similar with the outbreak of a restaurant with air conditioning in Guangzhou, China.21 In this article, the authors concluded that the most likely transmission was done by droplet and also emphasized the direction of air flow.*
This lines up with other studies I’ve seen which show that contact and fomite transmission do not significantly drive transmission (that means hand washing and surface disinfecting won’t make much difference).
Why would indoor dining be “safe”? Indoor anything is “unsafe”, as aerosolized transmission has been proven. Anything under a properly worn N95 doesn’t stop aerosols, and if anything will promote aerosols.
The idea that wearing a mask from the time you walk in the door to the time you sit down is somehow affecting outcomes is insane. People should know that walking into a restaurant carries some risk of infection and a mask isn’t going to change that.
> Type I, I R, II and II R face masks are medical masks tested in the direction of exhalation (inside to outside) and take into account the efficiency of bacterial filtration. Surgical masks of this type stop the wearer from infecting the surrounding environment. They are not effective at protecting the wearer from airbourne diseases such as coronavirus.
> Type IIR face masks EN14683 are medical face masks made up of a 4 ply construction that prevents large particles from reaching the patient or working surfaces. Type IIR Face masks include a splash resistant layer to protect against blood and other bodily fluids. Type IIR face masks are tested in the direction of exhalation (inside to outside) and take into account the efficiency of bacterial filtration.
They are not designed or tested to stop inhaling large droplets, nor exhaling small droplets. There is no scientific evidence they prevent the transmission of COVID and they specifically disclaim as much.
However, properly worn FFP2, FFP3, N95 and other respirator masks are effective at protecting the wearer from viral transmission. That’s just not what most people are wearing outside a health care environment. And you can’t simply take them off when you sit down.
Well forgive me but I was hoping for more than a first hit from Google and apparent common knowledge.
Since you mentioned having read studies about airborne transmission and aerosols, I was hoping you could point me to one where they examined the masks and found them to be significantly worse than FFP2.
Because in this study presented, only the people in the direct path facing the infected person were infected, not everyone, so wearing even EN14683 IIR masks could seem effective.
My guess, and this of many doctors in my area, is that EN14683IIR are, in fact, enough (if properly worn etc). If that is not true, I‘d like to know - from a reputable source.
The thing is specifically not designed to stop coronavirus, and specifically disclaims providing any protection against coronavirus. That’s not an editorial, that’s the written scientific standard for the medical device.
If you could get people to wear them without making people think they were a panacea then there wouldn’t be a problem (it would be a “can’t possibly hurt” situation). Unfortunately that’s not the equation that we’re faced with.
I’m sure EN14683 IIR is somewhat better than nothing, perhaps shifting the odds of infection somewhat lower depending on the circumstance. But if people slap one on and then feel they can’t be infected while standing in a room with people outside their household, that’s a mistake.
I think it’s blatantly obvious looking at flu vs. COVID numbers that it’s not that the precautions people are taking are not totally ineffective, they are just not nearly as effective as we need them to be against COVID.
Source on aerosolized transmission being proven? The discussion you're replying to is suggesting droplet transmission which are larger than aerosols and do not require an N95 mask.
Indoor dining is definitely a terrible idea, but if it's large droplets and not aerosols then you should be much better off with indoor activities where you can wear a mask.
I did cite a source, it discusses aerosol transmission and also the predominant method of infection (upper respiratory tract where the virus binds to ACE2 receptors) which is likely why surface contact spreading isn’t a huge problem.
They don't drive the transmissions the way they do for flu or some forms of common cold but I've seen estimates that 5% or so of infections come from fomites. It's still worth washing your hands when you come home and take off your mask since it's easy, but it's not going to make much of a dent in the R0.
Other sort of masks actually do make a dent in R0. A cloth or surgical mask doesn't provide the level of protection a N95 mask does but they do seem to provide a protection factor of 2 or 3. Nothing you could call safe but enough to reduce the R0 of the disease very significantly if everybody used them.
Where does this 2-3x factor come from? I just haven’t seen any proof of that.
From a macro perspective, masks did not stop the 2nd wave in Italy and France and their mask compliance was the highest in Europe. I don’t think you can claim Italy just didn’t mask hard enough.
Flu cases, by comparison, are down something like 99% year over year. So it’s not like I’m saying masks and hand washing don’t work. They appear to work extremely well for flu, they just obviously have failed to stop COVID.
If you look at how fearful some people are to even approach someone who isn’t wearing a mask, but then immediately feel safer when the mask goes on, it’s not clear to me a better approach wouldn’t have been “masks do not work, if you don’t want COVID then do not gather inside”.
Well, you can can put masks on dummies and see what fraction of aerosols of different sizes they stop, you can interview people after an outbreak and find out what protective measure they took and whether they get sick. You can look at which regions introduced mask mandates when and see what statistical result that seems to give on the number of covid cases. There have been an awful lot of studies on this topic over the course of the last 3/4 year and I'm also taking into account a study the WHO did after SARS-1 on mask effectiveness in Beijing. I wouldn't neccesarily have thought beforehand that fraction of particles stopped would line up neatly with reduction in chance of getting the disease but it seems to, at least roughly.
EDIT: Oh, and there are animal experiments where they put a layer of mask material between hamster cages and see if it prevents infections in the other cage.
” You can look at which regions introduced mask mandates when and see what statistical result that seems to give on the number of covid cases. There have been an awful lot of studies on this topic”
...all of which written in the spring, when cases were declining across the northern hemisphere. Subsequently, we’ve seen cases go up around the world, and it doesn’t seem to matter much if they have mask mandates, high self-reported mask compliance, or not.
This guy has amassed a huge collection of plots documenting the lack of impact of mask laws on outcomes:
If it were contact based, this would mean that at least one other in the restaurant must have contracted it that was outside of the airflow path. Since this not the case, the most likely thing is that transmission was with the airflow.
Why is it that you are so certain about this being surface based transmission?
Look at the time of arrival/departure for the customers. Case A arrived before Case B and Case A left before Case B left. On both sides of the door (or any other surface), Case A would have touched it before Case B. Despite this, Case B spread it to Case A.
Yes, they tested everyone else in the restaurant and no one else was infected. If you are going to make specific critiques like this, you really need to read the article first.
{kind=link}
{kind=link}