“If you can buy an 80% chance of stopping a deadly pandemic for the cost of having to wear some silly cloth over your face, probably that’s a good deal”
The reason the CDC didn’t previously recommend face masks could’ve been because of a lack of RCT. But in order to do that, they would have had to expose subjects to disease without face masks which wouldn’t make sense. Goes to show there has to better ways for judging the viability of something without resorting to a strict binary of “do or do not”
> Goes to show there has to better ways for judging the viability of something without resorting to a strict binary of “do or do not”
It's not just a question of how to judge but who makes the judgment. Part of the point of the article is that wearing a mask seems like something you should be able to conclude is a good idea based on common sense; you shouldn't need to wait for an expert to tell you, and if the expert is telling you something that seems to conflict with common sense, you shouldn't automatically disregard common sense.
Not necessarily. Doctors are exposed to a different set of risks while on the job than ordinary people going about their business. And common sense already tells you that it's a good idea to take precautions when working with sick people, so the fact that doctors wear masks while ordinary people going about their business don't have to should not come as a surprise.
That's not to say that doctors (and others) can't have reasons other than "masks don't work" for recommending that people (other than other doctors) don't wear masks. Just that doctors wearing masks themselves, by itself, is not enough to know that their recommendation for ordinary people not to wear masks is unreliable. You need more information.
I disagree. I think the CDC did actually perform a cross-benefit analysis on masks during the initial segment of the outbreak. Given the not-incontrovertible, yet positive, efficacy of masks, combined with the implications of a PPE shortage for healthcare workers meant that there probably was a calculated decision made to not recommend masks. Though at this point, without some more transparency, I'm not sure what we can say about the CDC's decisionmaking here.
> not sure what we can say about the CDC's decisionmaking here.
We can say "gee, we should appoint more truthful bureaucrats".
It isn't a crazy guess that (for this pandemic) a useful mask for a normal everyday person is anything that puts something in front of their face that makes it a little harder to breath and baffles the air currents.
There may be a shortage of proven face masks but there is no shortage at all of things that could be sewn up to cover faces and deaden air currents. The cost is tiny vs the risk of it not working.
Officials who are more worried about preventing a response to the potential crisis than the potential crisis should not be in charge if there is a potential crisis. We want people to change their behaviors if there is a crisis. Ideally even before the evidence in overwhelming that there is a problem.
The cost of recommending masks is that a large minority of people will decide they need the best mask to protect themselves, and buy them up thus depriving the healthcare workers of them. Yes, in an ideal world, the entire situation would be spelled out and only those people who are truly at higher risk would acquire some of the limited supply of more-effective masks.
For that to work, however, requires a sense of community and level of trust in government that has been in short supply in the US in recent years. These factors were also in play for swine flu and the other potential pandemics the article examined CDC rsponses for. In a crisis, officials have to base their decisions on current conditions, not on what they should ideally be. Restoring trust in government is extremely important, but can’t be accomplished in the timescale necessary to be useful for this crisis.
There isn't a coach and team in the world, real or hypothetical, who could win a football game down by 10 goals with 5minutes on the clock. The mask stuff was deck chairs on the Titanic.
Agreed. There's a difference between "stop buying masks because we need to save them for nurses" and "stop buying masks because they don't help at all*".
Potentially, but then surely a Cost/benefit analysis would strongly encourage the CDC to stockpile them in advance too? Perhaps nations need strategic PPE reserves.
TFA actually mentioned that point specifically, if you read it...
> I went into it thinking they’d lied to us, hoping to prevent hoarders from buying up so many masks that there weren’t enough for health workers. Turns out that’s not true. The CDC has been singing the same tune for the past ten years. Swine flu, don’t wear masks. SARS, don’t wear masks. They’ve been really consistent on this point. But why?
That's very weak reasoning, and I felt it was more musing than anything else. What evidence do we have for it not to be true? Why do we think consistency with previous advice trumps scientific evidence here? It feels like a cop-out to rule out a cost-benefit analysis simply because this advice mirrors advice in the past.
>I think the CDC did actually perform a cross-benefit analysis on masks during the initial segment of the outbreak. Given the not-incontrovertible, yet positive, efficacy of masks, combined with the implications of a PPE shortage for healthcare workers meant that there probably was a calculated decision made to not recommend masks. (emphasis added)
You postulated that the CDC not recommending masks was due to a recent cost-benefit analysis taking into account a circumstance (mask shortage) that has only been true for a few months. The article and link shows that the recommendation predated that by 10 years. Ergo the mask shortage could not be the cause of that recommendation.
There's no reason to even think that the CDC considered recommending masks - surely the default position is to leave pre-existing recommendations (don't wear masks) in place. You speculated that they did an analysis, which is not in evidence, and made a conclusion based on factors that may or may not have been important even had the analysis happened. That seems pretty weak to me.
> There's no reason to even think that the CDC considered recommending masks - surely the default position is to leave pre-existing recommendations (don't wear masks) in place. You speculated that they did an analysis, which is not in evidence, and made a conclusion based on factors that may or may not have been important even had the analysis happened. That seems pretty weak to me.
You're right, there is a hidden assumption I have here that I did not document. I believe the CDC is, within human limits, a capable organization of experts. I assumed that it was more likely for an organization of experts to perform a cost-benefit analysis than simply reiterate advice given in the past under similar situations. If you disagree with this assumption, then that's where we disagree.
They did an effectiveness analysis at some point in the past. If the situation had not changed from that point in a way that would indicate masks should be used, why would they reevaluate the whole thing? No organization, no matter how capable or expert, has infinite time or resources to reevaluate every past policy every day.
You seem to think they looked at it, found evidence that masks were effective, but then decided not to tell anyone due to the shortage. But then, a few months later, while that mask shortage was still in effect they decided to reverse that decision. Which is completely irrational.
I'd say I'm assuming it's an organization like any other. You're assuming it's populated by maliciously irrational people who are out to get you.
> If the situation had not changed from that point in a way that would indicate masks should be used, why would they reevaluate the whole thing?
Changed from what? During previous coronavirus epidemics, the CDC did not recommend wearing masks, and during the earlier stages of the pandemic they did not either.
> why would they reevaluate the whole thing? No organization, no matter how capable or expert, has infinite time or resources to reevaluate every past policy every day
What... else would they be doing? The CDC's entire mission is to steward American public health. If they can't reevaluate in the face of a new threat, well, what good are they really?
> You seem to think they looked at it, found evidence that masks were effective
Yes, I do think the CDC is capable of performing a literature survey on masks. There have been several papers on masks, N95 or not, during previous epidemics. You can find several papers related to masks dating from the original SARS epidemic. Some of these papers were funded by the CDC themselves, so it makes absolute sense to look back at one's own publications.
> but then decided not to tell anyone due to the shortage.
I believe the CDC made a calculated decision based on an American population would hoard resources. In hindsight, some of this is occurring. Despite no actual shortages in production of toilet paper, flour, and yeast, there are shortages in supermarkets throughout the US, and I've heard anecdotes from friends' parents who decided to hoard masks, flour, and yest because they "were worried".
> But then, a few months later, while that mask shortage was still in effect they decided to reverse that decision. Which is completely irrational.
Guidance changes. Factors that go into updating your risk cost-benefit analysis (better understanding of transmission rates, political pressure, etc.) change over time, and an effective leader does not double down on previous decisions in the face of new information. There's nothing irrational about changing your position.
You've managed to argue with the individual phrases while missing the actual point.
Tell you what, let's assume that you're right. The CDC is continuously reevaluating mask usage by the general public, but recommended against it due to fears of a shortage and/or hoarding. That being the case, please help me understand the following:
1) Why did the CDC change guidance on mask usage despite the shortage and risks of hoarding being, if anything, worse than before? If it was the controlling factor before, why is it not a concern anymore?
2) If they are continuously reevaluating policies, and believed masks should be used, why was the guidance not changed at any point in the last 10 years when there was no shortage or any particular reason to worry about hoarding?
3) Why is this a more parsimonious or plausible explanation than the one advanced in TFA, which is that they had a very high standard of evidence which they have relaxed somewhat in the face of a pandemic?
It's actually the strongest form of logical reasoning, a formally valid argument. This argument is true no matter what you substitute for A and B:
* You said X did A only because of situation B.
* But X does A even in situation not-B.
* Therefore, situation B is not a necessary condition to cause A.
The only way to rescue "mask shortage" as causing the WHO's advice is if you can show that whatever caused the advice last time was missing this time, so the WHO was primed to reverse the advice until "mask shortage" brought it back to do the same advice again.
> It's actually the strongest form of logical reasoning, a formally valid argument
Garbage In, Garbage Out. You are making several assumptions in order to apply this "logical" (which logic? This isn't FOL, since FOL has no concept of time, so I'm guessing you're invoking some Temporal Logic) argument, you need to assume that the CDC is a static, homogeneous organization that, for the purposes of this statement, continues to be a valid X between the past and the present. This seems naive to me; the CDC has changed in funding, priorities, membership, and leadership over time, and it's unclear to me how you can use past behavior as an indicator of future communication.
As in: The CDC is a huge government bureaucracy that employs (and cannot swiftly fire) enormous numbers of people from diverse backgrounds. If RCTs aren't the standard, well then why not also wear crystals to ward off the virus? They're inexpensive, and they couldn't hurt-- you can probably find a poorly controlled study to support it too.
The CDC is not human, it is a meat-and-paper-political-machine. You cannot understand it's actions under the same framework you'd use to judge another person.
The CDC must contain internal defenses against hokum which are much stronger than any person needs to personally have.
So why does the CDC sometimes provide overly conservative advice even when doing so causes death? For the same reason the scorpion stings: it's in its nature.
It's far from clear to me that a CDC which did make a more prudent facemask recommendation would actually be a better organization overall. Sure, it would have gotten this one right, but it would have likely given other bad advice as a result.
>As in: The CDC is a huge government bureaucracy that employs (and cannot swiftly fire) enormous numbers of people from diverse backgrounds. If RCTs aren't the standard, well then why not also wear crystals to ward off the virus? They're inexpensive, and they couldn't hurt-- you can probably find a poorly controlled study to support it too.
Alexander's discussion of parachutes gave some good heuristics for when you should trust common sense vs require an RCT, which explains why his advice doesn't generalize to advocating crystals.
The heuristic was basically that you should trust common sense when
a) there's a solid scientific model of the key dynamics,
b) the purported remedy is cheap, and
c) the costs of not stopping the threat are disproportionately high.
Crystals meet b)[1] and c) but fail a) -- we don't have a validated model of crytal/virus interactions. In contrast, we know that (some) viruses (including this one) spread through unimpeded airflow, and masks impede said airflow. We know that high-speed impacts between your body and the ground are deadly, and parachutes demonstrably slow the falling speed of objects.
Thus, you should go with common sense in the absence of an RCT for parachutes and masks but not crystals.
[1] They might fail b) depending on the particular charlatan!
I strongly suspect that the virus doesn't survive in vitro when exposed to a multitude of crystals! A sodium chloride crystal, for example.
Due to placebo effect you could probably even extract a "reduces symptoms" in a not very good human study too.
:)
I don't disagree that you could setup a criteria which would admit masks and parachutes but deny crystals. But would it also deny all (or even almost all) other manner of 'obvious' snake oil past or future?
I didn't know there was such a thing as 'salt healing', specifically but just goes to show that if a thing exists then there is snake oil of it.
Your prior post asserted crystals might pass (b) and (c) but fail (a); my response was simply that I am not entirely convinced that it would unless a was fairly rigorous.
And what the CDC appears to be doing-- requiring a RCT-- can be seen as an extremely rigorous (a).
Sorry about the communications failure-- communication is hard. I appreciated your response, even if I apparently missed the point.
I was using "salt healing" and "crystal healing" interchangeably because you mentioned specifically sodium chloride crystals.
And I don't see a communications failure; you're communicating your idea fine, it's just based on not having read, and misunderstanding, the heuristics the author advocated for "when to require an RCT".
>And what the CDC appears to be doing-- requiring a RCT-- can be seen as an extremely rigorous (a).
And once again, it's a poor handling of evidence, for exactly the same reason it would be to "not advocate parachutes for jumping out of a plane" until the RCTs come in. That can only "be seen as rigorous" if you ignored the very considerations the author mentions.
I'll just excerpt a characteristic portion so you don't have to go to the site:
>>Goofus started with the position that masks, being a new idea, needed incontrovertible proof. When the few studies that appeared weren’t incontrovertible enough, he concluded that people shouldn’t wear masks.
>>Gallant would have recognized the uncertainty – based on the studies we can’t be 100% sure masks definitely work for this particular condition – and done a cost-benefit analysis. Common sensically, it seems like masks probably should work. The existing evidence for masks is highly suggestive, even if it’s not utter proof. Maybe 80% chance they work, something like that? If you can buy an 80% chance of stopping a deadly pandemic for the cost of having to wear some silly cloth over your face, probably that’s a good deal. Even though regular medicine has good reasons for being as conservative as it is, during a crisis you have to be able to think on your feet.
Honest question, are there many people out there who find wearing a mask "silly"? Yes, they can be sometimes uncomfortable in terms of ease of breathing but to be honest I don't find them silly at all, they serve a purpose, just like an umbrella serves a purpose, it would be stupid of me to laugh of someone holding an umbrella while it's raining outside.
I haven't noticed any of my acquaintances saying that mask-wearing is silly.
But I have noticed many people not observing social distancing and stay-at-home requests. Perhaps if those people ignore the guidance because they're not convinced it's important, those same people would judge mask-wearing to be a waste of effort.
Perhaps another issue is people who have heard that wearing cloth masks mostly prevents you from getting others sick, and some of them just can't be bothered to make small sacrifices for the speculative benefit of strangers?
Lack of RCT is a crutch (in this case), the practical reason is that as hard as it is to get face masks now it would have been much harder if the entire population was scrambling for them in the early days of the pandemic and given the US size, purchasing power and worldwide visibility it would have made it more difficult world-wide - all Western countries did the same, de-emphasized masks as they were imposing a lockdown and are now emphasizing them when planning for gradual release.
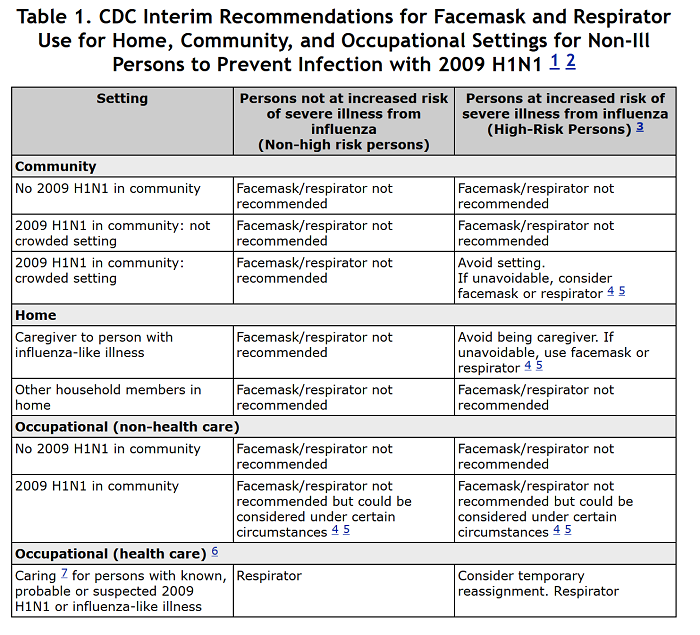
The article claims to refute your statement by pointing out that "The CDC has been singing the same tune for the past ten years. Swine flu, don’t wear masks. SARS, don’t wear masks. They’ve been really consistent on this point. But why?" This text in the article has several links.
Seems pretty consistent with my point - if masks weren't believed to be effective they would not be recommended "if unavoidable" , a use / don't use recommendation is not the same as a scientific finding of efficacy - it almost always factors in an implicit cost-benefit analysis of exactly the kind SSC advocates for. Case in point - all countries are now recommending (and in some places legally requiring) masks and not because a bunch of RCTs were conducted in the last two months.
{kind=link}
The reason the CDC didn’t previously recommend face masks could’ve been because of a lack of RCT. But in order to do that, they would have had to expose subjects to disease without face masks which wouldn’t make sense. Goes to show there has to better ways for judging the viability of something without resorting to a strict binary of “do or do not”