As it happens, I currently have COVID. When I first noticed I was getting sick, I was scheduled to fly in the near future, so I got a rapid COVID test that delivers results in 15 minutes.
It was negative. I got another one, and it was negative too. I had thus intended to go ahead with the trip under the assumption I had a minor cold.
Later, a few days before I was to fly, I lost all smell and taste. Now I didn’t know what to think. I wasn’t particularly congested, and the loss of smell was total. I’d never experienced this before. Could both tests have been false negatives?
I delayed the flight (free of charge luckily, so no big deal) and got a test that had to be sent to a lab for analysis. A week later, the positive test result came back.
Take from this what you will. I'm not a scientist or a doctor and frankly there's nothing remotely intelligent I can say about the various tests out there for COVID. But if the rapid tests are as unreliable in general as they were for me, it’s sort of no wonder COVID is spreading like wildfire. I was very, very close to boarding a plane with an active case of COVID, and I would have if I hadn’t acted out of an abundance of caution.
Rapid tests are known to be unreliable and particularly have a high false negative rate. That's why all the guidance has been that rapid tests can be used to indicate infection but not rule one out, and none of the screening processes based on exposure and symptoms accept “but I also had a negative rapid test” as neutralizing a flag on any screening factor.
> I would have if I hadn’t acted out of an abundance of caution.
The bare minimum of caution with a rapid test is treating a positive as a true positive and a negative as an indicator that you need a regular test. That you understood your actions to be an abundance of caution demonstrates a failure to effectively communicate on some level (I'm not saying that you are culpable; the information is out there's but delivery is...mixed, even before considering how it is muddled by misinformation from various sources.)
I definitely think there's a communication deficiency or breakdown happening, because none of the medical professionals indicated to me that the rapid tests were that unreliable when it comes to producing false negatives. I also feel personally guilty for not having been as well-informed as I should have been. I'm just glad I experienced a tell-tale symptom (loss of smell/taste) and was able to act on it before boarding a plane.
Another interesting aspect of this is that prior to experiencing loss of smell/taste, I was more or less told by urgent care staff that I didn't have COVID, and they were pretty resistant to testing me -- hence I only got rapid tests. Yet I actually was right in the midst of an active case.
> Are they just flat out missing some infections, or do they require a much higher viral load to indicate positive?
they do require a higher viral load than the pcr test to accurately show infection. the pcr test studies have shown to be 0-30% false negative later in the illness after symptoms have shown (when there are fewer antigens in the body). both the pcr and the rapid tests are expected to have a near 0% false positive rate though with most false positives being lab contamination or mishandling. even if the test is 50% false negative(not the actual number) it would still drastically slow the spread of the virus coupled with other measures. This is more of a defense in depth instead of a firewall; the swiss cheese layers of threat reduction.
That's true, but in this case the converse statement is also true that someone with a positive rapid test should start isolating even if symptoms are absent. It's this latter statement that you were replying to.
> because none of the medical professionals indicated to me that the rapid tests were that unreliable when it comes to producing false negatives.
You're being very emphatic about this, but all you've described is that the rapid test failed in a single case (you). We expect a lot more failure than that from the slow test! Where is the idea coming from that you experienced egregious unreliability?
Well, he did take two rapid tests, which both produced false negatives.
What this tells us about false negatives depends on details he didn't mention, about how correlated the two tests were. Obviously, it was the same person each time - but was it the same day? Same test brand? Same clinic? Same tester?
I've had 2 nasal swab tests. The first one seemed to have taken a core sample of my eyeball or brain; the second one was not as bad. I have no idea if these were rapid tests or googles PCR tests. Messaging is poor for sure.
I can't count the number of communication breakdowns any more with Covid. Apparently to get any number of people on the same page about something is not possible. Even with the internet. Blame it on information overload, or perhaps apathy.
I hope when Biden takes office he does daily Covid briefings where they disseminate accurate knowledge which would include correcting previous things we thought we knew. I know democrats that actually watched the Trump briefings because there were actually intelligent people behind half the info. I think many people tuned out the moment he recommended injecting bleach - but there was still value in the briefings. It was something that I know a LOT of people actually paid attention to.
> I think many people tuned out the moment he recommended injecting bleach - but there was still value in the briefings. It was something that I know a LOT of people actually paid attention to.
This is an interesting comment re:communications and the messaging that reaches people. Trump did not recommend injecting bleach. He went on a rambling mostly incoherent recollection of a conversation he had where he was trying to learn what was being done. He was trying to sound smart.
His comments were all questions to the med experts. "Is there a way we can do something like that?" "Are we going to check on that?"
Yet everyone jumped on it saying he "claims" or "recommended". And it became "truth" because news articles covering the press conference used phrases like "claims" and "recommended".
> "So I asked Bill a question some of you are thinking of if you're into that world, which I find to be pretty interesting. So, supposing we hit the body with a tremendous, whether its ultraviolet or just very powerful light, and I think you said, that hasn't been checked but you're gonna test it. And then I said, supposing it brought the light inside the body, which you can either do either through the skin or some other way, and I think you said you're gonna test that too, sounds interesting. And I then I see the disinfectant, where it knocks it out in one minute, and is there a way you can do something like that by injection inside, or almost a cleaning? Because you see it (COVID19) gets in the lungs, and it does a tremendous number on the lungs. So it'd be interesting to check that. So you're going to have to use medical doctors, but it sounds interesting to me, so we'll see. But the whole concept of the light, the way it goes in one minute, that's pretty powerful."
Presumably, Trump had been briefed about all of these things before giving the "inject bleach" press conference. The press conference is not the time to be asking questions you just thought about of medical experts. Not if you are the one giving the press conference at least. That is where the messaging fell apart.
Especially with the internet. In the 80s the main media outlets reported the page and almost everyone followed. The internet now has a million “experts” for every actual expert, and even good opinions can doffer depending how you look at the facts.
I'm glad the OP made the correct decision in this case and hope they get well soon.
> the assumption I had a minor cold
> the loss of smell was total
Since there does seem to be a messaging problem about the reliability of testing, I think it's worth emphasizing: if someone has symptoms of COVID, they should proceed as-if they have COVID. CDC guidance[1] is to isolate if you have a positive test OR if you have symptoms.
To do otherwise is to gamble with the health and lives of the people they meet, and the people those people meet, and so on. It may prove almost impossible to show who caught COVID from whom, but that doesn't mean that ignoring guidance won't lead to deaths. A statistical death is still the death of a real person, even if we can't put a name to them.
To be clear, the order of events was such that I did not have loss of smell/taste at the time of the rapid tests. There was no indication at that time of anything that wasn't completely consistent with and expected from a cold, and I even encountered resistance when I tried to get tested prior to the tell-tale loss-of-smell symptom appearing (hence the rapid tests only at that point). I had a mildly uncomfortable phone call with an urgent care center where they discouraged me from pursuing testing because they didn't think I had enough symptoms.
I knew exactly from whom I had contracted whatever illness I had, and that person had also tested negative for COVID (upon further questioning, their test had also been a rapid one, and they too had not been informed of its unreliability for any negative determination).
> There was no indication at that time of anything that wasn't completely consistent with and expected from a cold
Unfortunately, I think these days symptoms of "just a cold" are enough reason to self isolate for long enough to reliably get through the Covid incubation period - which locally (Sydney .au) has been reported to occasionally be as long as 10 days or more.
The USA currently has nine million active cases. I actually think at this point if you have cold symptoms it may be more likely you have covid than a common cold.
(Though maybe someone has data in cold cases to clarify the cross over point)
> The USA currently has nine million active cases. I actually think at this point if you have cold symptoms it may be more likely you have covid than a common cold.
Your intuition is wildly off-base here. Nearly all of us catch at least one cold a year, mostly during the winter months. There are, quite literally, hundreds of millions of colds a year. There's also ~half a dozen viruses in circulation at any given time that cause cold-like symptoms, vs. one for SARS-CoV2.
The steps we are taking to reduce COVID spread also reduce the spread of the cold. I would be absolutely shocked if we don't end up having our lowest impact cold and flu season in decades this year. That isn't to say the grandparent comment is correct, just that you can't really use a comparison from prior years as an indication of how many people will get a cold this year.
In the first 6 months of 2020, Australian influenza deaths were down over 90%, attributed to Covid anti measures - mostly increased hand washing/sanitising, social distancing, and school closures.
If we assume that's representative of a 90% reduction in flu and cold cases (not guaranteed, but probably a reasonable estimate to reason about), then perhaps instead of "hundreds of millions" of cases, it might be down to "tens of millions of cases" of cold/flu. So maybe 9 million Covid cases means any cold/flu symptoms are somewhere between 50% and 10% likely to be Covid - a virus currently killing ~1% of the people it infects.
I am certain the prudent thing to do in 2021 is assume _any_ cold/flu symptoms are likely to be a virus that's quite capable of killing you (and/or the people around you) and act accordingly until you are 100% certain it's not. (Which probably means 2 negative PCR tests ~10 days apart.)
> The steps we are taking to reduce COVID spread also reduce the spread of the cold.
...and cases are going up, so it's probably safe to assume that there are lots of colds being transmitted, as well. And as I said, there are many cold viruses in circulation, at all times.
Even if you believe that "the steps we are taking" are working, you have to assume that they're disproportionately effective for the common cold in order to make the statement the OP was making. Say what you will about SARS-CoV2, but it's more-or-less like any other respiratory virus in terms of transmission characteristics. There's no particular reason to believe that anything we're doing would stop rhinovirus or RSV, but not SARS-CoV2.
This doesn't follow at all because you are comparing the current state of laxing COVID precautions to the previous state of near zero cold precautions. For example, tens of millions of people are currently working from home and the workplace is one of the primary places colds spread. If we treated COVID like the cold we would already be on the other side of the pandemic because it would have already ripped through the population and millions would be dead.
> This doesn't follow at all because you are comparing the current state of laxing COVID precautions to the previous state of near zero cold precautions.
I am not. There are, right now, 5-6 cold viruses in common circulation. There is one SARS-CoV2 virus.
Nothing we are doing would be expected to suppress other respiratory viruses, but not this one.
>I am not. There are, right now, 5-6 cold viruses in common circulation. There is one SARS-CoV2 virus.
Yes you were. In your first comment you said "Nearly all of us catch at least one cold a year, mostly during the winter months. There are, quite literally, hundreds of millions of colds a year." Those are numbers in a normal cold year. This isn't a normal cold year.
>Nothing we are doing would be expected to suppress other respiratory viruses, but not this one.
I'm not sure where this line of argument came from as no one was arguing against it. The assumption is that these COVID precautions are equally effective against the cold, flu, COVID, and other similar respiratory diseases. This will lead to a huge drop in those non-COVID diseases as the precautions we are taking are so drastic compared to a normal year.
> Yes you were. In your first comment you said "Nearly all of us catch at least one cold a year, mostly during the winter months. There are, quite literally, hundreds of millions of colds a year." Those are numbers in a normal cold year. This isn't a normal cold year.
You can divide the number by any factor you want, but there are still ~6x the number of viruses out there causing colds. Even now.
>there are still ~6x the number of viruses out there causing colds
The variety of viruses is totally irrelevant to the original question of what are one's odds of having COVID based on having cold symptoms. The only piece of information that matters for that are the aggregate numbers and aggregate numbers from previous years are misleading.
> The variety of viruses is totally irrelevant to the original question of what are one's odds of having COVID based on having cold symptoms.
It is an essential factor, unless you make the (implausible) assumption that we have essentially eliminated all other respiratory viruses except for SARS-CoV2.
I like how you cutoff the my quote at the exact point that shows you how you are wrong. As I said "The only piece of information that matters for that are the aggregate numbers".
Whether there is 1 version, 6 different versions, or 1 million different versions of colds is irrelevant to your odds of having COVID when you show symptoms. What matters is whether there is 1 person, 6 people, or 1 million people with colds. The variety is meaningless. What matters is the aggregate number of cases.
> The variety of viruses is totally irrelevant to the original question of what are one's odds of having COVID based on having cold symptoms. The only piece of information that matters for that are the aggregate numbers and aggregate numbers from previous years are misleading.
It is an essential factor, unless you make the (implausible) assumption that we have essentially eliminated all other respiratory viruses except for SARS-CoV2.
I catch colds roughly 7-8 times per year. It sometimes feels like I have cold symptoms more days than I don’t. I currently have cold symptoms. If I had to isolate every day I had a cough, sore throat, congestion, or sneezing, I’d be under house arrest most of the year. I think it’s vitally important that we have accurate COVID tests that can definitively distinguish a case of the cold from a case of COVID.
At the end of the day everything is a judgement call. In this case I believe you're an outlier, guidelines are usually structured for the general case. Should you specifically treat every cold like it could be COVID? Maybe not, but should somebody else who gets sick only 1-3 times a year treat every cold like it could be COVID? That seems a lot more reasonable.
Not to mention it is wise and courteous to stay home and avoid exposing yourself to lots of people when you are sick regardless of if its COVID or not.
Not everyone can afford to stay home with minor illness. Not everyone will be employed if they stay home and can't "cover" their days off with measly 40 hrs a year of paid time for such purpose ( if they have any paid time at all).
This issue existed long before COVID. COVID is spreading partially due to this issue. Many people have no choice but work to avoid homelessness and/or hunger.
You should be tested for primary immune deficiency, based on the frequency of your colds alone. If you do have primary immunodeficiency, it is treatable with subcutaneous immunoglobulin, in most cases. Either way, it is treatable.
I am personally on subcutaneous immunoglobulin for two rare immune-mediated neurological diseases, and I have not had a cold in over 3 years, when I would get them a couple of times per year. It helps tremendously.
These are the 10 warning signs of primary immune deficiency in adults:
Adults
If you have two or more of these signs, speak to your doctor about a possible Primary Immunodeficiency.
1. Two or more new ear infections within 1 year
2. Two or more new sinus infections within 1 year, in the absence of allergy
For the broader point, regardless whether or not someone is more likely to have a common cold or COVID given the same group of symptoms, I think the point stands that if someone has symptoms consistent with COVID they should proceed as-if they have COVID -- especially given the current case rate in US.
Are you sure? Do nearly all of us catch a cold _this_ year? I know the flu is way down this year due to covid-related behavioral changes. I'd be surprised if common colds are unaffected.
I agree with you, and that's largely why I wanted to share my story -- to illustrate that even without any tell-tale symptoms and multiple negative test results, you can easily still have COVID.
Thanks for sharing your story, it's useful to hear anecdotes. I also want to emphasize I was making a general comment and not intending a personal criticism.
The points raised by bigiain and mxcrossb are well-made, "cold-like" symptoms are COVID symptoms, the loss of taste and smell only occurs in some cases. CDC has a full list of coronavirus symptoms[1].
I fear that many are flying, socializing etc. when they are actually symptomatic (e.g. headache, sore throat) because they consider these minor symptoms, or perhaps they can just "hope for the best", but the severity of the symptom doesn't change whether or not someone is symptomatic.
The heck is the point of a test if not to confirm or rule out covid? He took two tests, came back negative and assumed his "cold or covid" symptoms were cold until he had reason to believe they were covid. Other than the tests sucking everything in the fact pattern is perfectly reasonable.
Any test has a certain percentage of false positives and false negatives -- in fact, you can likely tune your ratio of false positives to false negatives depending on what your priority is. On a community level, the statistics from testing are essential for monitoring the spread of a disease, but on an individual level a test can still give an incorrect result, so shouldn't be the only factor when making decisions.
For an individual, if they have a negative test AND no symptoms AND no contacts with known COVID-positive individuals, then they can proceed as-if they don't have COVID and take standard precautions. However, if they do have symptoms, then that might mean further testing is required.
For anyone interested about testing, this graphic is essential:
It shows the difference in test efficacy for different tests (rapid antigen, PCR, antibody tests) as a function of time from symptom onset.
Rapid antigen tests only have a narrow window of efficacy. If they come back positive, you likely have COVID, but if they come back negative you could still have COVID and could still be contagious.
This is also why many countries are requiring PCR tests prior to entry, because they are more effective than rapid antigen tests, although can also give false negatives, especially early after exposure.
In my opinion, the rapid test's greatest value is using it to screen asymptomatic people in a regular (daily or weekly) process. For example, a school would test a random sample of students each day. This could help catch any stealthy clusters. It's not perfect, but it's better than just looking for symptoms.
It's also subtle in that while false negatives are common, false positives are rare (very rare). But general public don't get that subtlty and assume "the test isn't reliable" so a positive means they're not infected.
Almost no tests in existence can confirm or deny particular infection.
Think of them (and symptoms) more as odds updater. If you have 20 minutes to spare this video [0] by 3 Blue 1 Brown is a brilliant introduction to the concept.
Whether a test is positive or not depends highly on what type of test it is, and when you are tested relative to symptom onset. You can absolutely be carrying the COVID virus but still test negative. Heres a paper with a handy chart: https://jamanetwork.com/journals/jama/fullarticle/2765837
I think you testing negative was a combination of the rapid test being unreliable, as well as getting tested early with respect to symptoms.
Thanks for your anecdote. When SF was doing better and the possibility of big outdoor events with testing on the door were something that was being discussed, I looked at rapid tests together with some friends and the accuracy is really appalling. People relying on this to "safety socialize" may be one of the issues making cases rise in California, the math adds up. Many people reached to the government saying they should stop sponsoring and advertising rapid test sites because the false sense of security may be really doing more harm than good.
One of the rapid tests that we considered has, as advertised by its own manufacturer, a 10% false positive rate on basically all the population, and a 50% false negative rate even on symptomatic individuals with high viral load. Do the math, but using that type of test in something like for example a 100 person event or a restaurant will result in people being turned out of the door daily even if they were not symptomatic, and at least one or two people with high viral load being admitted into your place. I can't find the link of the test now, but there's better data about how harmful rapid tests are when not used together with PCR testing, for example here: https://www.bmj.com/content/371/bmj.m4941 and here: https://asm.org/Articles/2020/November/SARS-CoV-2-Testing-Se...
That's why most countries that really thought this through require a recent PCR test result for admittance.
It's really not clear what benefits rapid tests have if you don't have a model for population behavior. I think at lest the SF government is only doing them to save face now that the cat is out of the bag.
> But if the rapid tests are as unreliable in general as they were for me, it’s sort of no wonder COVID is spreading like wildfire.
Many rapid tests are indeed not accurate[1] but they still serve a purpose, depending on the sensitivity and specificity of the tests[2].
For the rapid tests with high sensitivity and you get a positive result, it's highly likely you have COVID.
For the rapid tests with high specificity and you get a negative result, it's highly likely that you don't have COVID.
And the public health measures of testing / contact tracing ONLY works if testing results come back quick. PCR tests are neither fast nor cheap, so those are not as effective in prevention of spreading because you don't do those all the time (slow + expensive).
I only have data points for two different testing orgs, but in my area, GoHealth charges $250 for a rapid test, and Color charges $110 for a PCR test[0]. So it seems like that's flipped from what you're suggesting?
The Color tests can even come back in 8 hours or so, if you're not too far from a lab and the lab isn't overloaded. Not as fast as 15 minutes, and certainly higher variance, but much more useful than 72 hours people normally assume.
Regarding false negative rate, Hawaii is accepting some of the rapid tests (like the aforementioned GoHealth test) for pre-travel screening, which is concerning.
[0] These are both without involving insurance at all. It's possible, though, that the Color tests are partially subsidised by Google?
This rapid tests have a very high false negative rate. The result you get back should really be "You have COVID" or "You may have COVID, get a PCR test".
Most countries which require a test for entry stipulate it must be a PCR test rather than a rapid (antigen) test. I’m currently in Lisbon waiting for the results of a 24h PCR test in order to board a flight to Azores, for example.
Rapid tests are at their most accurate when someone is at their peak infectiousness. Accuracy declines swiftly before or after that.
So the use you made of them didn’t fit their ideal use case, as you used them several days before travel.
Even then, with symptoms, I am not sure they would be enough to rule out a positive. The biggest use of rapid tests is finding additional positives that would not otherwise have been found.
> A week later, the positive test result came back
Which country do you live in that it takes a week for the PCR test to come back? It's around 24 hours here and I thought that was the case in all developed countries.
I'm in the US. The test was taken on a Sunday evening at about 7:30PM, and the results were delivered via text message the morning of the following Friday.
My guess is there's a lot of variability in how long it takes to get results. I know folks who've taken the same test and they got results back within 48 hours.
There's a lot of variability, and it depends on how far you are from the lab the particular test center uses, how quickly the test center sends your sample to the lab, and how busy the lab is.
I've had two tests that came back in around 48 hours and one that only took 8 hours (US, SF bay area). 4.5 days seems pretty excessive (and frankly pretty useless) though!
They've been using these lateral flow tests in the UK quite a bit - particularly for university students returning home/to campus (or at least, that was the plan!).
There is enough knowledge out there about the various kinds of tests (PCR, antibody, antigene) and what they're good for and what they're not. It's perfectly understood that while rapid tests are, well, rapid, they're much less precise than PCR testing. However, they are often better than nothing (you can't give a PCR test to everyone who wants to visit relatives in a nursing home), so they serve to minimise risk, not to remove it. (They also have a tendency to be more likely to be positive while you're actually infectious, which is not the same thing as having symptoms.)
I really don't think we should be discussing personal anecdotes during a health crisis, when there's enough data around that we can actually look at.
You were probably not contagious during those first days (at least for everyone except your partner).The threshold for the rapid test is higher than what the PCR detects. The antigen test is highly reliable for catching contagiousness, not just any viral load. Michael Mina (Harvard Biologist) presents the data in a great way if you want to check.
There are many different rapid tests. Some are reliable and some are unreliable.
For the ones that are reliable (like Abbott's test), they are highly accurate at determining whether someone is currently infectious. So you could have been infected but not capable of transmitting to others yet. These tests would be highly useful for onsite testing, such as if airlines required a rapid test right at the airport.
The most common error with these tests is false application. Did you have someone else doing the swab? It has to feel like someone is poking at your brain.
Sure, I'm in my early 30s. I do believe I had a pretty mild case all things considered, and I'm pretty much fully recovered at this point but still plan to quarantine for another week.
What I experienced was basically indistinguishable from a mild cold except for the loss of smell and taste, which took over a week to show up after the onset of the initial symptom (a fever). While I know loss of smell can happen from non-COVID infections, I can say this is the only time in my life I've had a total loss of all smell and taste. I'm very fortunate that this total loss only persisted for a few days, and at this point based on my subjective experience my smell and taste senses appear to be normal again.
If you still have yet to test positive for COVID you may not have COVID. A loss of sense of smell and taste is a common symptom of a viral infection.˜ [1]
Yeah - so you should probably go to a political rally or concert or a nightclub or something!!!
:sigh:
This is awful advice for 2021. (Even though _technically_ it's correct.)
If you have a loss of smell/taste you should 100% assume you have Covid and act accordingly, get tested immediately, self quarantine for probably 14 whole days, and get retested at around 10 days.
If you have "mild cold/flu symptoms" you should assume you like;y have covid, and should get tested (not with a "rapid test") and self isolate until you get a negative result.
Truth is, even with no symptoms, you could have Covid. If you've been in contact with anyone who has cold/flu symptoms, or been to a place where someone with a positive covid test has been - you should get tested (and probably self isolate until you get a negative result).
Results: The baseline assumptions for the model were that peak infectiousness occurred at the median of symptom onset and that 30% of individuals with infection never develop symptoms and are 75% as infectious as those who do develop symptoms. Combined, these baseline assumptions imply that persons with infection who never develop symptoms may account for approximately 24% of all transmission. In this base case, 59% of all transmission came from asymptomatic transmission, comprising 35% from presymptomatic individuals and 24% from individuals who never develop symptoms. Under a broad range of values for each of these assumptions, at least 50% of new SARS-CoV-2 infections was estimated to have originated from exposure to individuals with infection but without symptoms.
Conclusions and Relevance: In this decision analytical model of multiple scenarios of proportions of asymptomatic individuals with COVID-19 and infectious periods, transmission from asymptomatic individuals was estimated to account for more than half of all transmissions. In addition to identification and isolation of persons with symptomatic COVID-19, effective control of spread will require reducing the risk of transmission from people with infection who do not have symptoms. These findings suggest that measures such as wearing masks, hand hygiene, social distancing, and strategic testing of people who are not ill will be foundational to slowing the spread of COVID-19 until safe and effective vaccines are available and widely used.
> Yeah - so you should probably go to a political rally or concert or a nightclub or something!!!
I don't recall saying that.
> If you have a loss of smell/taste you should 100% assume you have Covid and act accordingly, get tested immediately, self quarantine for probably 14 whole days, and get retested at around 10 days.
Did I say otherwise?
What I said was, if you lose your sense of smell and taste and then proceed to test negative twice for COVID, you may well not have COVID.
Rapid tests are right 80% of the time. Two rapid tests back to back are right 96% of the time. That means after 2 tests there's a 96% chance you don't have COVID, and a 4% chance you do. That doesn't mean you should tour your nearest retirement community.
You shouldn't go out anywhere if you're sick in the first place.
[edit] Even then, there's a 1% false positive rate on PCR, and a 4% false negative rate on 2x rapid test. Even at this point there's a 20% chance OP doesn't have COVID.
> Rapid tests are right 80% of the time. Two rapid tests back to back are right 96% of the time.
I doubt the false negative % for two tests on the same person at roughly the same time are uncorrelated. (For two reasons: It seems logical that they would depend on viral load, and/or other non-random factors; And if they were independent, we would be able to achieve arbitrarily high specificity by taking and processing multiple samples -- just three would get you >99% -- which doesn't seem to be happening.) So the false negative rate for two tests might be much closer to 20% than 4%.
> That means after 2 tests there's a 96% chance you don't have COVID, and a 4% chance you do.
This part is definitely not accurate. The real probability will depend on base rates and facts about the individual case.
I don't understand why we don't implement the isolation procedures of countries that have gotten this under control, following these procedures for both foreign citizens AND US citizens:
- When you arrive in the US, you either spend two weeks at a government approved hotel, at your expense, which is monitored by federal agents to make sure you don't leave your room. You pay for room service for two weeks to get food. This is what Singapore does.
- If you don't want to stay at the government hotel, you agree to let the government track your cell phone for two weeks to make sure you stay in your home, and randomly call you twice a day to make sure you didn't ditch your phone. This is what Taiwan does.
As a plus, all the hotels near airports would be so thankful for all the forced business to make up for the loss of travel business.
They should have been doing this for the last nine months.
Edit: And obviously combine these rules with a relief bill that helps the industries that are hurt by these rules, or you know, everyone.
We do that in Australia too and its worked great. (Well, except for a notable quarantine breach 6 months ago due to mismanagement.)
The problem is all this is closing the fence after the horse has already bolted. The average person arriving into the united states is less likely to have covid than a resident. Currently 2.7% of the US population is infected with covid19, compared to 2.4% of people in the UK, 0.9% in Italy, 0.2% in Canada, and ~0% in Australia, NZ, Singapore, India, China, etc.
Almost all new infections in the US come from domestic transmission.
Where did you get those numbers? I read this comment earlier today, quoted 2.7% to a friend later, then realized I didn’t know what the source was and dug up your comment again.
Google took me here[1], which says India is down to 210k active covid cases at the moment. For a country with a population of 1.366 billion, thats only 0.016% of the population currently infected.
Its possible India's covid testing isn't telling the whole story - but they've apparently done 178 million tests to date.
Yes; India is probably missing the occasional case here and there. But given their daily case numbers have been dropping quickly, they're probably finding most people who have covid.
If India's real number of active covid cases was 100x the official reported numbers, they still wouldn't have as many active cases per capita as the UK and USA.
With all Australia's hard border closures and mandatory hotel quarantine, we've still had the UK Covid strain get out into the community. A cleaner at a quarantine hotel caught it from a returned citizen in quarantine (they're still not sure how), and spent 5 days in the community while infected. So far, it looks like we got very lucky, and the only person they've found that she infected is her partner.
From my point of view, the US (and UK and India and many other countries) have a categorically different problem to Australia (and New Zealand and Singapore and Taiwan and a few other countries).
We've _largely_ got things under control in Australia. Most of our cases in the last ~3 months have been hotel quarantine, with worrying incidences of outbreaks where it's escaped from quarantine but been tracked back and identified. Sydney currently has 3 clusters, with about 200 locally acquired cases between them in the last 4 weeks. I'm pretty sure every single one of them has been contact traced back to it's source of infection - and that contact tracing has also proactively got forward to get a very significant percentage of close contacts of infected people contacted and tested, and the places they visited while infectious identified, contact traced where possible (lots of venues are required to have covid checkin so people can be contacted an informed if they've potentially been exposed) - and any venues where they are not confident the covid checkins are comprehensive they publicise fairly widely and strongly encourage testing for anyone who visited during similar times.
This _only_ works because the numbers are so low. It all went to shit in Melbourne when a quarantine hotel breach happened and it got up over 700 cases a day, the contact tracing ability totally fell apart, and Melbourne went into a hard lockdown for several months to get it back under control.
In the US? Our approach just won't work. The virus is out and prevalent in your community. You have no hope of comprehensively contact tracing all of your positive cases, or identifying and mitigating all the venues they were in while infectious and contacting all the people who are at risk of exposure. The scale of your problem is totally insurmountable using the tools that work for us. If vaccination and/or herd immunity doesn't work out soon? You people might be totally fucked. ~1% of you will probably die from the virus, and quite likely a lot more will die from your medical system breaking under the load.
Sadly, I suspect it's like gun control. (I know, I know. Touchy subject, but hear me out - and please accept that I'm not trying to attack gun owners here.)
In Australia, there are few enough guns that reasonably strict licensing for owning/keeping/selling guns _mostly_ works. We managed to restrict "assault style" weapons early enough to have been able to do it before the prevalence of semi automatic weapons made it impossible. Gun violence here is several orders of magnitude lower that in the US by any reasonable measure. Not zero, but rare enough that "gunshots heard" is still newsworthy here.
If the US decided to try and get to that - it'd be a multi generation process to change attitudes and perceptions, and then to remove all the weapons currently in circulation. I don't believe there's the political or social will to even consider starting that. Your solutions to gun violence are fundamentally going to be different to Australia's.
(From my perspective, the news that my nieces regularly do "active shooter lockdown training exercises" in schools was inexplicable and horrifying. I kinda understand your historical "right to bear arms" - but I can't bend my mind into understanding how that's ended up at "there's nothing we can do about disgruntled teenagers getting hold of AK47s so we'll just teach our children how to hide under school desks and not make any noise, hoping that 'playing dead' will help them avoid getting shot". Not that I'm claiming too much moral high ground here, the most recent mass shooting in New Zealand was by an Australian. We have our fair share of fuckwits here too. Our main advantage is that most of those fuckwits do not have access to firearms when they fly into a murderous rage.)
I think is a case of a little too late. There's probably a higher risk of a traveller coming to US leaving with it, than arriving with it - currently. If this had happened 9 months ago, there might have been a chance of this working - with better leadership in other areas - as other child comments have pointed out.
> I don't understand why we don't implement the isolation procedures of countries that have gotten this under control
I'd hazard a guess that it's because they don't want to completely kill off tourism, an industry which is hurting pretty bad because of covid (see TSA arrivals screened https://www.tsa.gov/coronavirus/passenger-throughput)
No tourist would be interested in coming over to stay two weeks on their own dime locked in a hotel, only then to be able to do some actual traveling.
I have family and friends in the US. A lot of friends. I've visited on average 2 or 3 times a year over the last 20 years or so. (Almost all "tourist" travel, maybe 10 or so "business trips" for conferences or vendor meetings, all of which had ect4ended time as a tourist visit included).
I have accepted the fact that I'm unlikely to see my family or friends there for probably at least 3 maybe 5 years.
They will very unlikely be allowed to visit here (Australia), and if they are will probably need to spend 14 days in quarantine upon arrival. Right now I am not allowed to leave the country (without a special exemption, which sure as hell does not get granted "to visit my little sister and her family!")
Even if I got that exemption, I'd need to join the huge queue of people attempting to return to Australia with severely limited inbound international travel capacity (we were only allowing 4,000 returning citizens per week, with the current concern overt he UK strain that's been cut to 2,000 per week). There are news reports of people who've been trying and failing to get back to Australia for 6 months or more, with flights being cancelled - and confirmed tickets of flights being cancelled (reportedly for people with higher priced tickets to fly instead...)
I hope the vaccines work out. I fear that they may not - either being less effective that advertised, being less effective against mutated strains, or being thwarted by anti vaxxers.
I spent New Years weekend in Palm Springs going on day trips to Joshua Tree National Park. It was PACKED. The park is absolutely beautiful and everyone should check it out sometime. It's an almost alien landscape.
My hotel was full as well in Palm Springs. The only thin open late and popping was the Indian casino. They did check temps and make sure people had masks, but otherwise it felt like Vegas on a normal busy weekend.
Considering how many immigrants and children of immigrants live in the US, even if the people you saw seemed very diverse they could maybe have been primarily US citizens not foreign tourists?
The anecdotal evidence says that a small number of people have been reinfected, out of millions. Statistically, the average person is likely immune for at least a matter of months, probably a couple years or more.
It's definitely a thing - a couple days ago I've read an article where they did interviews with three people who got reinfected here in Czech Republic. It also mentioned a fourth person who unfortunately died due to being infected for the second time.
So even for a country with just 10 millions of people you can still find enough people who had covid twice to interview - how we fucked up the second and third wave notwithstanding.
> It's still not clear if a previous infection stops you from being an asymptomatic carrier, and we don't want more asymptomatic carriers.
It's as clear as it is for any other viral disease. For example, to my knowledge, nobody has ever done any kind of systematic study of whether or not infection with influenza protects you against asymptomatic reinfection with the same strain.
This is a level of paranoia that is unique to this particular virus.
> level of paranoia that is unique to this particular virus
This particular virus is >5x deadlier than seasonal flu, is significantly more contagious, and nobody has any pre-existing immunity.
Despite strong countermeasures, almost half a million people in the USA have died from the pandemic so far, and by the time we are through that number could potentially double.
It is the worst infectious disease threat since the 1918 flu (thankfully not quite as deadly as that one, given modern medical care).
Regardless, as I said before, demanding that some kind of study be provided to prove that asymptomatic infection is prevented by natural immunity is so far beyond what we know about any other virus that it borders on the hysterical.
This virus is significantly worse than the 1957 or 1968 flu, causing many more hospitalizations and deaths despite much stronger countermeasures. But those two were indeed quite deadly, worse than seasonal flu, and if a similar flu emerges in the future it should be treated extremely seriously. Hopefully we can learn from our severe systematic mistakes in the Covid pandemic to better prepare for and react to future pandemics of flu and other pathogens.
The 1957 flu had less than half the IFR of Covid. It infected a smaller percentage of the world population than Covid is likely to, despite much less significant public health countermeasures, and a tremendous increase in medical knowledge in the past half century. It was likely significantly less contagious.
Death estimates in the USA are in the 100k range, vs. Covid which has already killed more than 400k (if we count using a similar estimation method) and will likely kill at least 200k more before it is through. (US population has more than doubled in the mean time, but we are talking about at least 5–8x as many deaths.) The difference in hospitalization rate is dramatic.
It is really tragic that the abject failures of the US federal response have made partisans so heavily invest themselves in the claim that Covid is no big deal and we shouldn't worry about it.
> Globally, the 1957 flu caused about 1M excess deaths. Currently, Covid is attributed to ~2M deaths
No, this is a disingenuous apples-to-oranges comparison. One is a post-epidemic estimate by independent epidemiologists, while the other is a confirmed-positive-death count subject to contemporaneous political pressure and institutional inability to confirm every Covid death.
The contemporaneous confirmed death numbers from any seasonal or pandemic flu are always many times lower than the final estimate, and decades ago it was probably at least an order of magnitude lower. The discrepancy won't be quite as dramatic with Covid today, because a tremendous effort has been made around the world to get Covid tests to hospitals. But it will still be a very significant undercount.
After a couple years once experts have had time to gather and crunch the numbers, the number of Covid deaths from a comparable kind of best-guess estimate is going to double or more. Even in the USA, we are probably missing on the order of 150–200k Covid deaths so far from our confirmed death counts. And the situation is broadly comparable in Europe. But many less developed countries have much less capacity for gathering and reporting accurate numbers, and only a tiny fraction of Covid deaths are being reported in many places.
> One is a post-epidemic estimate by independent epidemiologists, while the other is a confirmed-positive-death count subject to contemporaneous political pressure and institutional inability to confirm every Covid death.
...as well as almost certain over-counting due to extremely liberal criteria for "Covid deaths" (e.g. deaths within 30 days of a positive test, which is the standard in many areas.)
Point being: there's uncertainty on the "confirmed-positive death count" in both directions and you're assuming that it's a strict lower bound.
Just today, the WSJ published an excess-death study that put the number at 2.8M, worldwide (or 3.5/10,000):
Higher than the JHU numbers, but still within reasonable statistical error of the 1957 pandemic estimates.
> After a couple years once experts have had time to gather and crunch the numbers, the number of Covid deaths from a comparable kind of best-guess estimate is going to double or more. Even in the USA, we are probably missing on the order of 150–200k Covid deaths so far from our confirmed death counts.
Well, now you're just making things up. Also, again: see the WSJ study above. Even if you count every excess death this year as Covid...it's about the same as the 1957 flu season.
covid-19 is not 5 times deadlier than the flu. It is about twice.
The IFR sits at ca 0.19. Flu is about 0.1.
Covid scare-mongers using inaccurate and outright false data to cause panic, terror and so much confusion that the public is left to choose what to ignore and what to follow, are causing much more damage than covid deniers are.
The fear of going to the hospital among people with other ailments come to mind.
There was an article in Nature the other day on the 300% increase in stillbirths in UK due to lack of in-person pre natal care. Another delightful side effects of the extreme fear propaganda.
No one listened to the idiot deniers anyway. They never were the problem.
0.19% is much lower than even the low bound of consensus scientific estimates; the Ionnidis paper on which he bases these estimates has also received significant direct criticism. In my opinion Ioannidis is a disingenuous hack who has thoroughly discredited himself during this pandemic, and from what I can tell his agenda-driven Covid punditry is popular on Fox News and Breitbart but not taken seriously by professional epidemiologists.
The US CDC's best estimate of IFR as of a planning scenaario document from September was 0.5% for people aged 50–70, and 5.4% for people aged 70+. (This is not the best source available, but miscellaneous journal papers could be criticized as cherry-picked.) Adjusted population IFR varies from place to place, depending on the proportion of seniors, people with pre-existing health problems, access to medical care, etc., but nowhere in the US is it as low as 0.19%.
If you want a credible widely cited meta-analysis, try e.g. https://link.springer.com/article/10.1007/s10654-020-00698-1 from December which calls Covid "far more dangerous than influenza", and estimates the IFR to be at least 5–10x higher.
> The estimated age-specific IFR is very low for children and younger adults (e.g., 0.002% at age 10 and 0.01% at age 25) but increases progressively to 0.4% at age 55, 1.4% at age 65, 4.6% at age 75, and 15% at age 85.
> As shown in Fig. 6, population IFR (computed across all ages) ranges from about 0.5% in Salt Lake City and Geneva to 1.5% in Australia and England and 2.7% in Italy.
> Supplementary Appendix O: [We estimate that during winter 2018–19] the population IFR for seasonal influenza was in the range of 0.04% to 0.08% – an order of magnitude smaller than the population IFR for COVID-19.
* * *
> increase in stillbirths in UK
The UK has royally screwed up most aspects of pandemic response. Just like Brexit and everything else the Tories have had their hands on in the past few years. You don't see the same problems in other wealthy island nations like New Zealand or Taiwan.
(With the notable exception that the UK has done a decent job sequencing a large collection of viral samples.)
> Across 51 locations, the median COVID-19 infection fatality rate was 0.27% (corrected 0.23%): the rate was 0.09% in locations with COVID-19 population mortality rates less than the global average (< 118 deaths/million), 0.20% in locations with 118–500 COVID-19 deaths/million people and 0.57% in locations with > 500 COVID-19 deaths/million people. In people < 70 years, infection fatality rates ranged from 0.00% to 0.31% with crude and corrected medians of 0.05%.
But this is a meaningless debate. Your own preferred source makes it clear that the "average IFR" is heavily dependent on population demographics (i.e. in the very next sentence after the one you quoted:
> our results indicate that about 90% of the variation in population IFR across geographical locations reflects differences in the age composition of the population and the extent to which relatively vulnerable age groups were exposed to the virus
You're also completely misinterpreting Figure 6 from that paper. It is showing that their model of age-specific IFR correlates well with observed differences in reported IFRs. It is not claiming that those reported values are meaningful in the absolute -- in fact, all of the "reported" values seem to be higher than the model by a factor of ~2-4, and they're substantially higher than the numbers cited by the WHO bulletin.
(and yes, I know you don't like Ioannidis, but this is a metareview, not original research. Also, not liking someone doesn't make them wrong.)
Still doubt that that many people will travel long distance because of the hassle, the risk of getting stranded or having to deal with the local overwhelmed health system. Anecdotally I know a couple of people in Europe that travelled quite a bit during summer because it was an unique chance to see some historical places e.g. in Italy without the mass of tourists they are usually overrun by. But that was a tiny fraction of the usually very travel happy social circles of mine.
But for the US I think the main attractions are the big cities and the national parks. The former are not really tempting to go to atm and the latter you usually want to go in groups and they seem so vast that I don’t think it is that big of an opportunity to go there when there are few tourists. The only people I know that traveled in between continents in the last months did so for family reasons and it was a huge pain for everyone with multiple flight cancellations, chaos with ever changing immigration requirements that not even the officials can keep up with, self-isolation, etc.
Speaking as an Australian, I'm not allowed to travel to the US at all right now, unless I'm moving there permanently. Keeping everything open (and thus keeping covid rates high) isn't doing your international tourism sector any favours.
> No tourist would be interested in coming over to stay two weeks on their own dime locked in a hotel, only then to be able to do some actual traveling.
Depending on where they're coming from they'll have to do that on the way home, so they're not interested in coming anyway.
Before you get on the plane you need a negative test, but even then there is a mandatory 14 day quarantine. When you arrive you are required to have a SIM card. During quaratine, they track your device and call randomly one or twice a day to be sure your phone is on you. Breaking quarantine is a big fine (up to $33k USD) and there is a carrot if you complete quarantine without any incidents ($500 or something?). Individuals are provided quarantine housing if they can't pay but employers are expected to pay (e.g, workers from Indonesia).
I assume this is combined with some kind of mandatory GPS tracking. The GPS tracking knows the phones location and the call confirms the user is next to their phone.
They were not asleep, they were deliberately letting the car drive off a cliff because they thought admitting there was a cliff there would make them look weak.
Probably also contributed by the fact that the opposition pointed out that they should avoid the cliff so the only option left is to intentionally drive off it.
Also (to extend this metaphor to all three modes of transport), they were sure that - should any cliff present itself - the greatest nation on Earth will not fall down it, but will boost off and fly towards the sunset.
Would you agree with the court when it determined that the rights of black people were different between northern and southern states, or that internment of the Japanese was legal during WWII? The supreme court has been wrong on many issues for decades on end throughout US history. They haven't all of a sudden become infallible in the last 20 years.
If you're hinting that what is legal is not necessarily right, it seems odd to fall back to this position when the original comment about the 1st and 5th amendment are legal, not moral.
Instead of just mentioning the 1st and 5th amendment, it may have been better just to say that the US has a culture of privacy and personal freedom.
> The Supreme Court has already ruled that neither of those apply at the border. Nor does the 4th.
reply
This is an extremely overbroad generalization.
The supreme court may or may not rule that forcing someone to be surveilled by federal agents in order to travel by plane is unconstitutional, or it may not. And it may be right or wrong. My qualm is legal and moral.
>I don't understand why we don't implement the isolation procedures of countries that have gotten this under control, following these procedures for both foreign citizens AND US citizens:
I know its probably crazy to ask, but tell me where in the US Constitution does the federal government have the power to force me into a hotel at my expense
I know in "times of emergency" people seem to think the constitution is suspended and the government as "unlimited power" but last I checked Emperor Palatine was a fictional character, and saying "Singapore does" well Singapore is an Authoritarian nightmare IMO, one i do not really want to replicate here in the US. I pass taking public policy lessons from Singapore
It's part of protecting the borders. The Supreme Court has already determined that anything within 100 miles of the border is the "border zone" and gives the government broad authority to enforce border protection within that zone.
Also, it could reasonably argued that it is part of their "protect life" job.
That is a stretch of the reading of those provisions, the court has generally (and wrongly IMO) allowed Federal Law enforcement to stop people with in the border zones to establish if they crossed the border illegally, once Citizenship is established then normal protections snap back into place
Even at border crossing the government has been allowed to seize Devices and other things but they generally can not prevent a US Citizen from entering, they can stop you from bringing your stuff, but they cant stop you (outside the limited questioning detainment certainly not 14 days) unless they have an arrest warrant or some other cause of action to arrest you
Pandemic+unknown disease status is proof of danger.
You can argue that isn't a high enough standard, but it's a pretty clear one, and given the exponential spread, it's a real actual danger that can be controlled at the point of entry.
Given that Virus and Biology have no obligation to be compatible with various national and international laws, it is upon human society and governments to work around the virus.
Thus, for e.g., people in South East and Far East Asia learned from the earlier pandemics and voluntarily wear face masks to protect themselves and those around them even when one has "just a cold or a cough".
People also agreed to socially and physically distance when asked. The messages from scientists and doctors have been enough proof of the dangers that the virus poses.
That is fine, my problem is recently we have just be ignoring the constitution when it is deemed to be a problem
The fact remains the federal government has no constitutional authority nor do most state government.
If we need "pandemic response" authority then we need to amend the constition to add the power to the government not just simply declare it so because "The Experts™" have declared that is what is best for us.
if that is the measure of our rights, we have no rights at all. If rights can be stripped with a simple declaration of emergency, on which there is no power to challenge that declaration then we have no rights at all
To believe the government will not use this unprecedented event for which they have usurped a wide range of never used before power in ever increasing ways is naive and ignores all of human history.
It will not be long before the seasonal flu or cold will be enough to warrant draconian measure and limited on personal freedoms, or be used for privacy invading policies like contact tracing all the time (which will then be used for Law Enforcement like in Singapore)
it amazes me out people can not see what is next, or maybe than can but simply believe the promise (false promise) of safety is more important than liberty
Personal attacks are not cool here, regardless of how wrong someone is or you feel they are. We ban accounts that do that. If you wouldn't mind reviewing https://news.ycombinator.com/newsguidelines.html and taking the intended spirit of the site to heart, we'd be grateful.
Edit: looks like we've had to ask you this more than once before. Please don't do it again!
This was not a personal attack. This was an attack of their position.
A: "We should be doing [stupid thing] X"
B: "Good thing you're not the one deciding."
B is not a personal attack. The entire premise of the point is that it's because of what they said/think, not something personal about that particular individual.
> That is a stretch of the reading of those provisions
Any, you know, the government and law enforcement have _never_ been known to do that...
"It's not 'collection' if we permanently record every phonemail/textmessage/email ever sent. It only counts as 'collection' if a human reads/listens to it!"
Borders (and airports) are already a constitutional twilight zone. Just to get into (or sometimes out of) one I have to go through an X-ray scanner or manual groping that on its face would violate the Fourth Amendment. But at the same time, nobody is forcing me to go there.
A similar requirement has been enacted in Canada and what has happened is that Canadians with covid can't return home to Canada and are stuck abroad.
It really gives some teeth to the "do not travel" recommendation - if you get covid abroad you can't come home until you test negative. If you get covid at home and then go abroad you can't come home until you test negative.
I think people who previously would have travelled and just risked it will be a lot more careful now since they can't get home if they are sick with covid. Instead of dozens of flights per day entering canada with covid cases we now have zero [1].
Small correction: you can't board a flight to Canada. You're always welcome at a land border without a test report in hand. In which case you'll be required to spend 14 days in government quarantine.
You spend the 14 days in quarantine either way - land or air. And it's not 'government quarantine' for most people - it's just a hotel room, airbnb or wherever your approved plan says you're going to quarantine.
"As has been the case for months, all travellers will have their quarantine plans reviewed by a government official and, if not suitable, will be required to quarantine in a federal quarantine facility."[1]
Canadian citizens and permanent residents always have a right to enter. Presumably if you come to a land border without a negative test, you won't be trusted to self-quarantine properly and will be whisked off into a federal facility.
I think it's highly dependent. I came to Canada a few months back, completed the Federal and Provincial quarantine plans. All I got at immigration was a "be careful" and 2 calls from the province asking if everything was ok.
I've heard that that is generally the case. I was merely pointing out that if you show up at a border crossing without a negative test despite it being required, you likely won't be trusted to "be careful".
>I'm totally ok with covid19 positive Canadians being stuck an unable to return home until they test negative.
I am not; your home country should never deny you entry. You're telling a citizen he is not welcome in his own country, is that how you want to treat your citizens?
Quarantine is warranted but denying entry has a weird taste to me
It's an imperfect solution. But thousands of people have left to the beach in Mexico, Florida, etc. We aren't talking of people that got surprised by COVID in March, we are talking of people that bought a plane ticket in the middle of the pandemic, traveled abroad for vacation, and are now inconvenienced by the fact they need to get tested to come back.
I'm also in the same situation with my home country. I was born there, has the country passport, don't mind 2 week quarantine, commercial airlines have expressed interest but they are simply not allowed. Only a pitiful amount of repatriation flights are done.
I can't believe it's harder to go back to my home country than to get a visa to the US. I'm lucky I can stay long-ish term in the US but many many others are screwed.
I understand the country is underequipped to deal with a lot of people coming back and it's better to protect many more people inside but I do feel forgotten sometimes. What's the point of having the citizenship then if I can't even come home?
I’m assuming this is Vietnam as I have friends going through the same issue. Citizens of Vietnam and they are on a 6-9 month waiting list for a repatriation flight with the gov’t basically saying “if you can stay where you are you can’t come here”.
They can’t even even pay for a commercial flights and quarantine like other countries.
And because Lunar New Year celebrations are coming up, repatriations flights have been cancelled until after as they are concerned with all the travel within the country.
There's a big problem of Vietnamese who are stranded and jobless in Japan -- they lost their (mostly travel-related) jobs, cannot pay tuition, and cannot return home:
I guess the situation with Vietnam is more unique that I thought.
This is an unrelated rant since the absurdity of the situation got to me. If you can hear the rumors about the reasons why there are fewer repatriation flights in January though, it definitely takes the cake.
I am terrified of the possibility of this being retained after the pandemic and expanded to cover other maladies. There already is a concept called medical inadmissibility, but it only applies to foreign nationals. It really concerns me that we are not applying it to Canadians as well.
There are labs that guarantee < 72-hour turnaround times for travel. It costs extra but hey, that's life. This pandemic has been around for a year now so if it was that important to travel, it's worth paying extra for the test.
Not every place in the world is going to have PCR tests with results in a 72 hour window. There are going to be lots of Canadians falling through the cracks.
The 30 minute tests are antigen tests. The 72 hour tests are PCR tests. Antigen tests can basically only detect the virus if you're currently contagious. PCR tests can detect the virus before and after you're contagious. Airlines typically require the 72 hour PCR tests.
I don't think you need an 8 ball to predict that you shouldn't travel during this global pandemic -- especially in the past 6 months when it's all hit the fan.
Now they are in countries in the Caribbean that have managed the virus relatively well and are overloading their public health system because they urgently need tests. Canada is just creating a problem for poorer countries while gaining very little - there's barely any community spread. If a Canadian returns home from the Carribean, on average both countries will have less covid.
Governments has been telling people for months not to go on vacation, that is correct, they should have thought of that before leaving.
They also gave 2 weeks notice so if you went somewhere and didn't think you could get a COVID test, there was still time to make it back home before the ban started.
If only these people would suffer that would be alright - it was their mistake. But rich countries should not make poorer countries pay for the bad decisions of their own citizens. Policy needs to be guided by data, not emotions.
Keep in mind individuals can test positive for months after being infected but are not at risk for spreading the virus. It really should be a negative test or 14+ days after a positive test.
my friend's father passed away from covid three weeks after contracting it at a curling tournament which they obviously shouldn't have held, even in a small town in the middle of nowhere. he was 65 years old and had just retired. being dead is also not cool.
Only 2% of cases are coming from outside of the country, so this seems mostly like a political thing than actually being useful. There's a lot of lower hanging fruit to get a 2% reduction. This seems too heavy handed in places where it's not currently possible to do a 72 hour test.
At the very least give some options to those can't meet the requirement. These people have to quarantine two weeks after returning anyway - I just don't see the logic behind this move.
> These people have to quarantine two weeks after returning anyway - I just don't see the logic behind this move.
Well, presumably a lot of the people taking foreign holidays are covid sceptics. So expecting 100% compliance with all quarantine rules would be pretty naive.
totally ok with letting them get stuck abroad. It's weird that everyone is freaking out about people travelling when the airports remain open and the guidance is totally about what ppl do inside the country. If you must keep the airport open(IMO should close them), let people leave and don't let them come back. If they leave, it's their problem (and unfortunately, some other country's). Stay at home.
There are risks to traveling internationally, especially during a global pandemic. Getting stranded at your destination happens to be one of them.
I know a woman who traveled from the US to Trinidad last February to care for her mother. She is still stuck there today. Fortunately, she has internet and an understanding employer.
I recently had to get a negative COVID result to travel to Hawaii to see family. Hawaii only accepted tests from a very limited number of providers which complicated things, but after some effort I made an appointment and got a test. The rest of the process was very painless. We all had to keep masks on for the entire flight of course since there was no requirement that we all have a negative result before getting on the flight but it was comforting to know that nearly everyone else on the flight would have had a negative result so as to avoid the mandatory 14 day quarantine upon arrival.
If you enter Mauritius you have to get four tests in total over several weeks. Islands are taking advantage of their isolation to get this pandemic under control.
Madeira has been very successful during all of 2020 with not letting it escalate.
I don't at all see how this is relevant to the United States in 2021, when COVID-19 is almost completely prevalent, and we require universal vaccination to exit out of the pandemic - International travel restrictions seem meaningless to me now - though they would have been invaluable in January 2020, and maybe even February 2020 - right now the major risk of COVID-19 infection is inside the United States. A handful (or heck, even hundreds) of people coming into the country won't make any difference when we have thousands of new cases a day regardless.
There's a reason Epidemologists don't put much stock in travel restrictions once a pandemic is well underway around the world - they don't do much good.
But - generally, having widespread (ideally very sensitive) COVID testing for any type of travel outside of the home is a good thing. We should have it universally available. Ideally <$10, something that everyone could do weekly, or even daily if they travel a lot.
Just unclear what the focus on international travel is all about here.
Some rationale for blocking international travel - preventing the spread of international variants, and preventing the destination country from being overloaded by incoming infections.
Most nations aren't getting the vaccines yet. Vaccination distribution and delivery require complex logistics. Nations that don't have a good public healthcare infrastructure need time to gear up. Vaccinations have just started and are being given in a phased manner. Blocking International Travel (or at least mandating a 14 day quarantine) helps keep variants in check.
Ironically, it's in countries where there is partial vaccination that we haven't the greatest risk - partial pressure against the virus will select it for stronger ability to be vaccine resistant. It's why it's so important to give everyone two doses of vaccine as quickly as possible and vaccinate the entire population, so you don't have the virus spreading, mutating, and potentially evolving to become vaccine resistant and then endemic in the population. We only get one really good chance to hit herd immunity.
But - longer term - agree with you - wouldn't it be awesome if we had full-viral scans of travelers, international or otherwise - would shut down flu pandemics as well (most of them are imported from other countries).
I think all domestic and international travel should have this requirement at a minimum. Nobody should be on an airplane without a recent negative test. Or working in a factory, hospital, or other indoor environment for that matter, it would be great if essential workers could all routinely get tested once or twice a week, though maybe that's not feasible.
I don't really get the international focus of this either, but it seems like a step in the right direction.
This is no surprise, although according to CDC research, this only reduces the infection rate among these passengers by 5-9%.
A lot of EU countries require their own citizens of their countries to get a COVID-19 PCR test prior to entry. A lot of times, this has to be paid out of pocket abroad.
What research is this? As far as I've been able to tell, CDC hasn't conducted a single randomized survey on any large group, but has only collected convenience samples.
Also keep in mind that due to compounding (keeping these people from infecting others on the plane and at home), the effect extends beyond the people prevented from traveling. You can also speculate that detectable infections are more transmissible during the journey.
Anecdote from a German that visited Spain to see the family: Spains government requires <72h old negative covid test before entering the country, with 6000€ in fines if no test can be presented. Also, a form about symptoms etc had to be filled out.
After arriving at Valencia, Spain, there was a big line where we had to show the form's result QR code only. Not a single passenger was asked for the covid test.
I've heard that the vaccine doesn't make you less likely to transmit COVID - just less acute symptoms. So getting the vaccine doesn't really help other people - just you. From this perspective, this doesn't make much sense (unless the objective is to make $ for the corporations).
You heard wrong. Nobody actually knows if you can transmit after getting vaccinated or not. Thus far anyone who claims otherwise is a liar.
There is some evidence that some of the vaccines prevent transmissions, but we need more study before we can make a statistical determination.
We know why other vaccines have failed to stop transmission. The reasons those vaccines didn't stop transmission do not apply to the covid ones. However there is a lot we don't know about biology so until we have better evidence no expert will state that the vaccine stops transmission even though many believe it will.
It was just published today that in Israel, where around 20% of the population has already been vaccinated with the first dose, they're beginning to see clear evidence that vaccinated people do not transmit it others.
Tests weren't widely available a year ago. 3-6 months ago maybe.
In fact a year ago, exactly, the existence of COVID was still being denied or downplayed by the Chinese government. Very few people in the US even knew about it, and only if very plugged in to Chinese social media or non government sources.
I'm pretty sure it was being widely covered (and acknowledged by the chinese) in late January during Chinese New Year. https://www.nytimes.com/2020/01/29/world/asia/coronavirus-ch...
At the time the US evacuated ~200 people from Wuhan, flew them to LAX (well, landed at a nearby air force base), made them stay in isolation, then monitored them as they returned home for 2 weeks.
I think the times reported (in a serious article) that China reported the first death on or around that date (https://www.nytimes.com/2020/01/10/world/asia/china-virus-wu...). I certainly recall seeing coverage of it before that although it was very muted.
"There is no evidence that the new virus is readily spread by humans, which would make it particularly dangerous, and it has not been tied to any deaths"
Clearly, between Jan 8 and late Jan, was the time of massive increased interest, so we're not really in disagreement.
It was on my radar in mid January; I know this clearly because it made me choose not to buy plane tickets for a big family celebration scheduled for the end of February.
Well I'm talking about the 12th, China was rounding up and arresting doctors talking about it and making them sign apology statements. You might be thinking of a week or two later.
The USA was doing 500k tests/day back in May, and over 1m tests/day by July. Probably couldn't have happened earlier than that, but it would definitely have been feasible mid last year.
In order for a policy like this to be workable, you need tests to be widely available in the countries people are travelling from because the whole point is to test people before departure - and they simply weren't in most non-US countries.
Per capita it's really most of western Europe and the US that are struggling, and the US is doing better on vaccinations so far while it has had a higher case and death rate than most but not all of Europe. It's rather misleading to just cite a total confirmed case count.
There are only a handful of countries not western Europe or the US where I would trust their numbers. Of the list Vietnam is the only surprise.
Trust means their official numbers within a reasonable margin of error of correct. Nobody have perfectly accurate numbers, but the ones are trust are generally not miscounting by enough to worry about.
Just to clarify, the linked article isn't really talking about false positives. It's talking about people who are carrying the virus, but perhaps aren't contagious due to it being only small amounts.
"False positive" isn't really an accurate term there.
If there's no virus, you're not going to be able to amplify it. A too-high threshold may detect non-contagious levels of virus (still a concern, if you're in the early pre-symptomatic days of an infection) or non-infectious virus particles left over post-infection.
Not really, no. They specifically pick genomic sequences believed to be unique to SARS-CoV-2; they're specific enough to distinguish between SARS-CoV-2 and the other known coronaviruses, let alone less related viruses.
This article doesn't mention PCR tests, so perhaps we're being smart enough to accept the often-more-relevant-for-infection-control antigen tests for this purpose. (I'd not yet bet on it, given how bureaucracies have made almost every wrong choice so far, but: maybe?)
But also: if PCR false-positives are a concern, the cycle standard can be reduced, or the reporting expanded to include the cycle on which a test turned positive, so that "positive" tests that are likely dubious/marginal/past-infection can distinguished from "blazing active infection".
The rapid antigen tests have a significant problem with false-negatives: the BMJ reported that Innova tests have 49% sensitivity.
That makes it pointless to use as a border control - for every two cases, at least one gets through. (Or, potentially much worse, under this system: I throw away my positive tests and show whatever false negative one I have).
You ideally want to be conservative and permit some false positives at an effective border control, because you don't want to risk infectious cases getting through and causing an untraceable national breakout.
Even tiny sensitivity would be better than nothing – or something that's so slow & expensive it's impractical.
But other antigen tests purport to have 90%+ sensitivity.
And the kinds of "PCR positives" they miss are often cases that are no longer infectious, anyway: lingering viral fragments, rather than live full-virus shedding.
So: ideal for border-control & creating other internal gradients that help suppress the worst active cases. The perfect should not be the enemy of the very good.
> Even tiny sensitivity would be better than nothing
Not if you imagine that one case on a plane = potential super-spreading event, the plane touches down and then newly infected people go in every direction.
Your hypothetical test with tiny sensitivity is pointless, in this regard: it has a (less than) tiny chance of preventing each risky passenger. In my view, any kind of low-sensitivity testing before departure is theatre: it won't make any difference in preventing new infection from breaking out.
The government of the country that I am in agrees, and requires a negative PCR test.
By now people can purchase negative Covid PCR test results at many international airports, sometimes for as little as $0.50. Entrepreneurial spirit is hard to tame.
This is moronic. We have between 30M and 130M cases here. There is no mathematically possible way in hell that international passengers could bring COVID here in any noticeable way at this point.
Why would they do this? I'll tell you the one and only one reason: some people are making tons of money off it. I just flew back to Hawaii from California and had to pay $170 for a COVID test, even though I'm already immune.
I think it’s more about protecting the passengers who are in an enclosed space together for 6+ hours than preventing spread within the US. I find it a big reassurance.
I get why they’re doing this, but I fear as a society we’ve learned the wrong lessons about testing.
These tests have a pretty high failure rate. That’s probably ok for social level spread tracking (with wide error bars) or low volume contact tracing (where quarantining a few extra people is worth it). It’s far better than nothing of course, but it’s also far short of what we expect from something like a pregnancy test.
But as a means to sign people off as safe to travel? Yeah, not so much. So many people have had the “one negative test so I can go party” only to discover what a false negative is.
Most US states already require a negative test or quarantine, with some exceptions. The only issue is that almost no one is enforcing it (maybe some airports do, I'm not sure). It makes sense if it becomes like visa where airlines wouldn't let you board the plane without it (until things are under control). It can be an issue for emergency travel though. Thinking about it, this should be of interest of airlines to protect their staff.
Right. Santa Clara County, California, has a mandatory 10-day quarantine for anyone arriving from more than 150 miles from its borders. This notice is posted in the airport but aside from that there is no framework for enforcement. It is not even all that easy to figure out what territory is outside this zone and the county does not provide a map.
Yea, we really should stop saying things like the government “requires” or “orders” something, if at the end of the day it’s not being enforced. No US state [EDIT except maybe Hawaii?] seems to have any kind of actually enforced public health rules around COVID besides business closures, where enforcement is spotty at best.
It's not clear to me how this works. What if you've recently recovered from a confirmed case of COVID-19? People can still test positive up to 90 days after recovery, even though all guidances say they stop being contagious 10 days from the onset of symptoms (assuming symptoms have improved and no fever).
And what about people who have been vaccinated. Wouldn't proof of vaccination be sufficient and spare limited testing capacity?
The vaccine question is going to be interesting. On one hand, if I'm vaccinated then I should be able to fly right? But no vaccine is 100% effective so do I need to get tested anyway? Are we just gonna have to get used to supplying a DNA sample every time we buy plane tickets?
A positive test result from > 10 days ago and a temperature check should be sufficient. Otherwise, we're just asking people to get tested over and over (and most guidances say don't get tested within a few months of a positive result).
But they'll let people in who have long term residency permits, or to visit long term partners, sick family members, or e.g. if their young children live there.
For Switzerland I know there's even a clause that lets you in if you have to go there for business. Kanye West was spotted in the country last month, I guess he was allowed in because he's building a villa there.
All countries have various levels of business travel, for example obviously all courier services and shipping still happens and other exceptions are made all the time depending on the situation. Diplomats can still travel. Kanye West can probably come up with a legitimate reason to travel to Switzerland even if he spends half his time on the ski slopes.
I don't know, even then, the "herd resistance" (not immunity) applies to new arrivals and residents alike.
Best advantage I see is perhaps plane ventilation is bad, but that would purely benefit other passengers and air transportation workers, not the general public. I doubt such narrow beneficiaries is their goal.
Not to be inflammatory, but why? The only benefit I can see is reducing the likelihood of new strains getting into the US, but to me this is like a swimming pool requiring people to be dry before they get in.
It would make sense as part of a national strategy, no doubt. But on it's own, I don't see the value in this?
Especially since it doesn't apply to passengers transiting through the US, so technically not everybody on the flight will have to do this, meaning you're going to spend a lot of time in an enclosed place with (as a complete guess) 80% covid negative people and 20% YOLO people. That's, err, that's exactly how covid spreads...
Actually, I would say this is more like taking a shower before entering the pool. It reduces the chances you are going to bring in grime into the pool.
Of course the pool itself is not very clean, but this way you improve the quality of the pool while you FINALLYYYYY put in some chemicals (vaccines) into the water.
Agreed 100% that this needs to be part of a national strategy in which testing, vaccine deployment, and strong community guidelines are used in conjunction to really beat COVID-19
That's an irony. USA is pretty much a fortress for as long as border security goes, and it had the best chance of any nation to avoid Covid impact by shutting itself off from the world using mechanisms of border security only.
Yet, for some completely unfathomable reason, it didn't.
You would need more than just a pre-travel testing requirement. You would also have needed an arrival quarantine and post-arrival testing.
I wonder what percent of asymptomatic positive cases pre-arrival testing actually catches. I’m sure that number also changes depending on how many days before traveling you’re allowed to get the test.
And to actually prevent COVID from entering the US, I think you would have needed all of that fully in place in January, or perhaps earlier.
Effectively what this would have meant is a total border closure for several months at the beginning of the year. I’m not sure if that would have literally been impossible, but I think it’s totally fathomable why that didn’t happen.
In January, outside of China (possibly elsewhere in Asia) absolutely everything was business as usual. I was traveling in Europe for 3 weeks at the end of January/beginning of February and everything was 100% normal.
The absolute earliest I could see significant shutting down in the US would have been early March which is when companies started canceling events, etc.
I don't have exact date timelines, but I know the large company I work for decided that the US was a coronavirus hotspot somewhere around the end of February and the beginning of March and banned business travel to or within the US. It was only in mid-March that they shut down the offices themselves, a couple of days before state or local governments began locking down.
I believe the current estimate is that there was uncontrolled community spread in the US by late February, and closing the borders to international travelers wouldn't have done anything to prevent its spread in the US.
I was at a relatively smallish (maybe a few hundred people) tech event in Phoenix the first week in March. There had been some consideration to canceling but they went ahead. They were cleaning surfaces, doing elbow bumps instead of handshakes but no masks, distancing, etc.
I was supposed to head on to another fairly small event in Tahoe the next week but the Thursday before, they canceled it. Which TBH seemed excessive to me at the time. (Though CA was starting to see an increase in cases.) I got home, did some shopping before everything went crazy but about a week later offices were closing, etc.
The Chinese were low key buying up as much medical supplies in Europe as they could get their hands on and flying them to China. This didn't raise any alarms.
The West displayed an enormous level of incompetence same as the Chinese authorities but you can at least understand why the CCP cadre in Wuhan was so negligent. There is something in the human brain that makes people incapable of recognizing danger until they experience it.
Australia has had these measures in place for a while now but quite a while after January and they work pretty well. I think one of the very effective tools Australia has is the ability to close borders with other states. In the US even if one state is doing pretty well, it doesn't matter because people from other states will come in and ruin it.
> You would need more than just a pre-travel testing requirement. You would also have needed an arrival quarantine and post-arrival testing.
Yes, and those are what US has in abundance, but does not use for some reason.
I believe every international airport has quarantine zones, and US has quite extensive TB quarantine infrastructure it could've reused.
Lastly, it could've finally put its incarceration industry to some good use.
It's very much like US found it had many months worth of PPE stockpiles laying forgotten in diffent institutions long after US spent hundreds of millions to rush order it from China.
But indeed this wasn't in place at the start of the pandemic, and New York's ability to enforce it is quite weak.
Do we know if the new US federal order will allow the unreliable rapid tests to meet the requirement? Canada's similar requirement, added last Thursday, insists on either a PCR test or an RT-LAMP test. Edit: the wording in the CDC's FAQ requires a "viral test (NAAT or antigen)". I guess that does include the unreliable rapid kind.
The UK is and island and they didn't do it either. It's learned helplessness: the world has given up on the idea that it's possible to contain the virus.
"We're testing all international travelers" is gonna be hard to tag that way. "We're banning people coming in from China but allowing in US citizens or permanent residents untested and unscreened on those same flights" looks pretty dumb from an epidemiological standpoint.
> “There’s no restriction on Americans going back and forth,” Klain said. “There are warnings. People should abide by those warnings. But today, 30 planes will land in Los Angeles that either originated in Beijing or came here on one-stops, 30 in San Francisco, 25 in New York City. Okay? So, unless we think that the color of the passport someone carries is a meaningful public health restriction, we have not placed a meaningful public health restriction.”
I don't really remember medical experts were saying in early 2020, but I would have supported banning specific countries if it was based on a framework that adjusted bans as the number of cases changed.
I remember being unimpressed with the timing, starting the ban right after the super bowl was over was a bad idea. And the US should have immediately started working towards testing all travelers.
When Trump banned China he put in all the press releases and announcement speeches that he also wanted to ban Mexico (0 known cases at the time). This easily led people to believe the whole thing was xenophobic.
Don't forget his earlier travel bans against primarily Muslim countries, excluding countries that he personally does business with. A history of xenophobic actions from Trump means that he reasonably lost the benefit of the doubt for later cases.
Only if implemented in an inconsistent fashion - where travel from some areas with high levels of COVID is permitted, while travel from other areas with much lower levels of COVID is not.
Which is currently the case. For example, travel from Russia to the US is currently allowed, despite Russia having >3 million COVID cases, but travel from Finland (>37,000 COVID cases) and China (>97,000 COVID cases) is prohibited.
It's not even a quid-pro-quo, because Russia has banned travel from the United States (>22,700,000 COVID cases, FYI.)
If you want to stop travelers spreading COVID in the US, the first thing you should do is ban domestic travel, and the second thing you should do is to update the travel ban to include infection data from any point past ~April 2020.
If you're not willing to require someone flying from New York to Nashville to have a negative COVID test before getting on an airplane, you probably shouldn't spend too much time wringing your hands over someone flying from Hanoi to LA without one.
> Which is currently the case. For example, travel from Russia to the US is currently allowed, despite Russia having >3 million COVID cases, but travel from Finland (>37,000 COVID cases) and China (>97,000 COVID cases) is prohibited.
China is doing great if those numbers can be trusted.
But Finland having 80x fewer cases when they have 25x fewer people isn't a big enough difference that I would say "much lower levels".
Finland's not exactly a COVID-free paradise, but my point is that there is no good epidemiological reason for a travel ban that includes it, but excludes Russia.
Which leads me to believe that the current travel bans have been made based on arbitrary political, rather than science-backed epidemiological reasoning.
The first person would, most of the time, not bother making the drive, which would have the same mitigating effect on COVID transmission.
The real reason for why domestic flights don't require negative tests is because it's politically inconvenient for the government to ask for them, and because it would gut airline revenue. "Controlling the spread" plays second fiddle to matters of political expediency and money.
That, and it's much easier to impose restrictions on foreigners, even if, as of January 2021, those restrictions don't accomplish much.
President Trump has never shied away from xenophobia from the day he announced his candidacy [1] to today when he gave a speech in Alamo, Texas [2] What Trump has done is try to minimize public concerns about COVID-19. [3]
The relationship between border towns is very tight. You would ruin the entire southern economy if you banned cross-border travel entirely.
Back in the day before Mexico required passports to enter, many people lived in Tijuana and worked in San Diego. I'm sure this still happens today, and of course, you have to consider that many migrants work in US farms, etc.
San Ysidro is still the busiest border crossing in the world. It's nominally 'closed', but still open for trade. In normal times you don't need a full passport, either- just a passport card is fine, and realistically a CA driver's license will get you through without trouble. It kind of has to be that way- Tijuana and San Diego are far too closely tied together for much else.
Border closures don't have to be all or nothing. In Australia we closed borders between states but allowed work permits in some places and had fuzzy borders (people within 100km could cross) in others.
The US has two huge land borders that people regularly commute
and trade across (not to mention cross illegally).
The only success stories with this strategy are Australia and New Zealand, which are island nations completely isolated from anywhere else.
Even single breaches of their 100% quarantine of all arrivals caused outbreaks, and they also closed state borders.
This requirement begins to make sense now there is a vaccine, as within the US the curve should bend down vs the rest of the world, without the vaccine it wouldn't have achieved anything.
> The only success stories with this strategy are Australia and New Zealand, which are island nations completely isolated from anywhere else.
I don't know why it is ignored, but Vietnam (population 90M) is a large country with many land borders, including a border with China, and it has done spectacularly well containing the coronavirus.
Not to take anything away from the island countries but having no land borders makes limiting the influx of Covid much simpler.
I don't know much about Vietnam's borders and how much crossing there was in pre-Covid times but perhaps it should be the Covid success model that all non-island nations emulate.
The land border with Canada has been closed (at the Canadian government's request) since March. Only trade is allowed, no personal travel at all. So, no, I don't think it's impractical at all. Trump did complain a lot about us closing it, though.
Air travel, however, has been permitted all along, and mostly from what I can tell because of the fact that the airline industry would go bankrupt otherwise. So there's still people coming into Canada from the US constantly by air, and likely breaking their 14 day quarantine period, too. I know of some
personally.
International travel is still being promoted heavily by airlines, despite governments giving official guidance to not go. Big scandals here in the last couple weeks about politicians taking off for tropical vacations, after instating tough lockdown rules and telling the public not to travel.
Canada also instituted the negative test on arrival rule in the last week or so. The caterwauling from our airlines was just ridiculous.
The federal governments in both Canada and the United States failed to make moves against travel early on, and they just let it coast for months, as if this virus was just going to go away on its own, because they were afraid of bankrupting the airlines.
> Canada also instituted the negative test on arrival rule in the last week or so. The caterwauling from our airlines was just ridiculous.
The negative test requirement is only for air travel, and in spite of your assertion, there is (limited) non-trade travel allowed across the border. I'm driving across the border in a few weeks, and for some reason don't need a test that I'd need if I flew.
you can close land borders just as you can close air borders. the threat model is average joe unknowningly carrying the coronavirus on their vacation / business commute, not some special op team sneaking into the country.
> The only success stories with this strategy are Australia and New Zealand, which are island nations completely isolated from anywhere else.
Taiwan is another such success story (7 deaths total, zero domestic cases for over 200 days) and it's not exactly that isolated from, well, the place where the pandemic started.
It was. A sensible policy would have restricted all entries — at the time Trump restricted entry from China, there was no credible reason to believe that it hadn’t spread elsewhere.
> Yet, for some completely unfathomable reason, it didn't.
Let's not forget that President Trump's order for closing the borders with even just the source nation of the contagion was labeled by the incoming President-elect as xenophobic[1]:
>> "We are in the midst of a crisis with the coronavirus. We need to lead the way with science — not Donald Trump’s record of hysteria, xenophobia, and fear-mongering. He is the worst possible person to lead our country through a global health emergency."
Covid testing hasn't been, and still isn't, universally available. Mexico, to pick one neighboring country with a lot of cross-border traffic and cultural ties to the US, has done 97% fewer tests than the US has, for example.
> The only question is why this wasn't done as soon as travel was restarted
I'm not sure there was a point where travel was ever _stopped_? At least not for US citizens or residents. This is not to say the test requirement should not have been imposed (much) earlier, however!
testing capacity couldn’t support it. no use doing this when the results come a week later. if this was a requirement earlier everyone would have complained it was just theater and not helping
Maybe politicians should bite the bullet sometimes and do stuff that will not be immediately understood by every citizen.
Even without tests being widely available it would have been wise to require all arrivals to quarantine, as Taiwan has done with great success.
Yeah, sure, that would have been a nuisance for quite a few people and painful for the airline industry, true, but nowhere near as annoying and painful as things have ended up now.
India has had this requirement for a long time now (more than 6 months IIRC). If you don't have the negative test, you need to quarantine at preselected hotels near the airport after arrival. Most international airports now also offer on arrival tests.
In most countries they just want a negative test from the origin country, so the country being visited doesn't have to spend a test for the tourist. But it's not bulletproof, if someone tests false negative and flies and infects a few others.
Other countries (Taiwan, NZ?) quarantine you for 14 days on arrival, and also test you...
NZ currently requires a negative test if you are coming from the UK or US as well as 14 day quarantine for arrivals from anywhere (with more tests). You can also only return if you are a NZ citizen or permanent resident or you get some kind of special dispensation (notable recipients of these include film crews and America's Cup sailors).
I’m certain we could have figured out something earlier. We spend several billion dollars annually on an organization with a singular mandate to do so.
This doesn't make any sense. Requiring a test on entry to country with full-fledged epidemia is like asking for an umbrella on entrance to the swimming pool.
I recall that the science deniers were the ones in favor of border restrictions. Besides, I don’t envy anybody whose position is so weak they must resort to finger pointing. A scientist would let the data speak.
It’s clear through this all that we’ve seen great power wielded. Regardless of who you support, I hope anybody reading this remembers that there are more important things than winning. The government has a monopoly on violence. It doesn’t need you that much. Our kids are the losers when we allow ourselves to be pitted against each other.
They based border restrictions on bigotry, not science. And the cost to wait and collect more of that data is time and corpses, so it's not so cut and dry.
Just so silly. More theater. We're already seeing millions of new cases per week including the strains with mutations to the target spike proteins - what problem does this solve?
In order to stop seeing "millions of new cases", every source of new cases should be reduced.
International travel is an orderly place to apply a filter, just as hospitals test all admits (even those without symptoms).
Blocking all visitors from specific places – even places with lower rates of prevalence than here! – was silly theater. This is actually well-targeted to reducing the interactions of the likely-infected with the uninfected.
(If a city or state/province even wanted to set up internal borders, & require on-the-spot quick antigen tests to enter regions of actual or attempted-infection control, perhaps even anonymously, that'd also be a well-targeted intervention far better than the other theater we've been fed so far.)
Even in expensive hospital systems in the SF Bay Area, it's not every patient getting a test, much to the chagrin of some of my friends working at the ones that aren't doing universal testing.
Well, it would've decreased the chances of a more infectious strain becoming widespread in the US if it had been implemented months ago. It could decrease the chances of worse strains that might originate outside the US becoming established moving forward.
Sure they can, but reducing the geographic spread would reduce the chances of those randomly occurring variants spreading quickly around the world. I would expect other countries to require testing of international flights for the same reasons.
The US is performing badly when it comes to controlling the virus, but it could still get significantly worse.
All of the research on masks published before it became a political issue said as much. The general public doesn't wear masks properly enough for masks to have an infection control effect.
Interesting, what exactly are they going to do if someone doesn't have one? IANAL, but as far as I recall from "what if they want you to unlock your phone/mount your encrypted drive/... on the border and threaten to not let you in" articles that purported to be written by lawyers, they cannot not let a citizen in.
Answering my own question... CDC page has better information - https://www.cdc.gov/coronavirus/2019-ncov/travelers/testing-... this is basically at the point of departure, so the airline won't let you board in the first place, and the awkward issue of not letting citizens into their own country won't arise.
Most places in the world don't have reliable means of getting a test done within the 3-day return time. I guess when I go visit my family abroad, I am going to fly back to somewhere like Tijuana, cross the border, then fly domestic back home. I'd encourage as many people as possible to do the same.
This appears to only be required for inbound passengers. I wish it was also required for outbound. I not only want to prevent more COVID from coming into the country, but also want to increase the chances of my outbound flight being COVID free.
The infection rate in the US is so high that the average arriving international traveller has a lower chance of being infected than the average US resident. What exactly is the point of this? Constitutionality aside, you would literally make a bigger impact on mitigating the virus spread by testing random people on the street. Like DUI checkpoints or stop-and-frisk but for covid.
They should have done this when there were far fewer cases. It was really surprising to hear that you don’t need any tests or quarantining when you travel from other countries. Better late than never, I guess.
Well, got to remember, when there were far fewer cases, tests were still in prototype phase, not widely available, and in some cases unreliable (I think a lot of the Japanese cruise passengers that got the WHO test tested negative, then later came down with it after being released).
Yeah, but we could have done more. There was a lot of supply chain issues the government just ignored. I remember in early 2020 when masks were unavailable a couple domestic mas manufacturers were saying they weren't comfortable producing more. They could scale up production, but they didn't want to deal with suddenly firing people when things went back to normal.
Didn't I just say testing wasn't reliable then, because it was very new? So it wasn't a long time ago. Reliable tests weren't available en masse until maybe summer, and even then not in all countries/areas.
India made tests mandatory to skip institutional quarantine on August 8th i.e. more than 5 months ago. That is sounds like a long time ago to me compared to when US has decided to make this a requirement.
Are these PCR based tests? What is the accuracy rate? I was told it is far from 100%.
So is it possible that someone might test negative but then is actually asymptomatic?
This is exactly what happened last year in South Korea. People were tested many times and they were negative but turned out they were asymptomatic that the test kit failed to pick up.
Nothing about the virus is going to be 100% effective. It's a matter of compositing things that are 60% effective and 90% effective and 50% effective.
If they require testing which is 80% effective, and masks which are 80% effective, and get vaccination up to xx%... etc etc. You eliminate vectors for the virus one at a time and eventually there aren't enough vulnerable people contacting each other in ways that are contagious.
It isn't even 80% effective from the scientific journals I've read last year, the best they can do is 40% and lower, I think there is some inherent limitation in its accuracy.
I'd like to point out that many countries aren't running multiple tests to make up for this low accuracy like South Korea. It is the general consensus among experts that the actual case numbers are far far higher than what is reported
So if the 40% rate is true then the law of large number suggests the screening test is completely useless because it misses the 60% of the time. It's just like the Casino where the virus has a huge edge over our detection and prevention measures.
Every time you block some percentage of spreaders, you are reducing the reach of the virus. Even if a measure is only 20% effective, it's worth investing in.
If it's 40% effective and masks are 40% effective, collectively they are 64% effective together. This idea that measures need to be 90% effective is bunk. Incrementally we can improve the odds significantly.
In most other situations I would agree with you but this virus has a transmission R0 of 6!!! [1] This means even if you block 40% that remaining 60% that slipped by will overwhelm your medical infrastructure like what's happening in Japan now who didn't follow South Korea's standards (out of pride? so many countries chose to ignore Taiwan and South Korea's advices in the early days).
This is why you have extreme disparity between countries like Taiwan, South Korea, Vietnam vs America, Europe, Japan.
40% doesn't mean you are catching 40% of the viruses here. It means your detection is only at 40% capacity, like your vision.
I'm arguing for multiple PCR tests spread out over a few weeks to make up for this low accuracy. I doubt many people will put up with it like they did in South Korea or Taiwan. Especially North America where the individual rights come before the well being of society.
I actually thought that North American and Europe were anti-fragile, this virus quickly proved otherwise. How do you force individuals to comply with rules that is designed for the greater good when they've been told all their life their individual needs come first and the rest of society has to accommodate them?
Even getting people to wear masks is still an issue. I'm utterly disillusioned after 2020, the racist attacks from both sides of the political spectrum, the misinformation built upon centuries of stereotypes and exceptionalism, and a politically divided environment to boot.
As soon as we get more data on the vaccine's effectiveness on dealing with mutation variants over 1 or 2 years, I am getting the fuck out of North America and taking all the jobs with me.
Because this isn't the first pandemic and it sure as hell won't be the last, and I highly doubt people will have learned their lesson. Conspiracy, memes, and other incompetent thinking that arises from laziness. People in North America and Europe have lived comfortably for a long time post-WW2, relying on economic hegemonies, military intervention, immigration to do the dirty work, and I believe they are in decline now. Sure America will remain #1 military superpower but front lines have simply shifted away from trenches to our minds where you can conquer and control how people think in foreign countries. This is what unrestricted warfare looks like and we are seeing the fruit of this labor to the delight of its enemies.
[1] I recall reading Dr. Feigl-Ding's twitter last year which pointed to an American journal that cited this figure back in 2020 but I can't find it right now.
Are you suggesting closing international flights entirely or tighter restrictions should be required?
I've just heard quite a few people suggesting that if some counter-measure isn't "good enough" we shouldn't bother with it. I thought that's where you were going with this.
I don't object to tighter measures or double tests at all.
Also, I understand what you meant by 40% effective.
> So is it possible that someone might test negative but then is actually asymptomatic?
No, with PCR, the opposite is true. It is most likely that someone who is "positive" but asymptomatic has such a miniscule amount of virus in their system that they're not infectious.
> the researchers presumed that 30% of individuals who contract the new coronavirus never develop symptoms but remain 75% as infectious as those who do develop symptoms.
They made up some numbers and played with the math. It's conjecture, not research.
The second definition from Wiktionary is most appropriate for this situation:
> (formal) A supposition based upon incomplete evidence; a hypothesis.
There is no evidence that asymptomatic people are 75% as infectious as symptomatic people. The 75% number was fabricated to allow them to build a model. Asymptomatic people could be 0% as infectious as symptomatic people. Or, by some unexpected turn of fate, they could be 200% as infectious as symptomatic people. The evidence doesn't exist.
Your link even mentions another scientist who believes that asymptomatic people are only 35% as infectious.
Long overdue! Really sad why this wasn't done earlier. Regardless of false negatives, this will certainly dent imported case numbers, though it would have had much more impact earlier on in the pandemic.
This seems like a scheme that will be ripe for gaming / outright fraud. How exactly does the U.S. verify anything? Basically the only way to do this would be to have control over some kind of verification system that comes from vetted and registered hospitals.
Even then you have so many problems. There is no realistic way to even partially guarantee that forgeries won't happen regardless of your vetting system. And add to that the fact that the U.S. government has no control over regulations in foreign countries, so there is no way to force validators into compliance.
A half-baked plan that will screen out only some COVID carriers is better than the status quo where we screen out none of the COVID carriers.
In Hawaii, they have limited partnerships and Hawaii verifies the result directly with the labs. It says on the website they'll prosecute anybody that submits forgeries, but it's true that this is much easier to do when everything is within the same country.
My experience flying from the US to France through Portugal was that an agent at the gate looks over whatever paper you give them and highlights "PCR", "NEGATIVE" and the date and then hands it back.
Then in Portugal they asked for the paper and waved me through, and the same at the French border.
So logistically, pretty easy to fake (unless you're stupid enough to be trying to buy the fakes in the airport like some guys who got caught in Paris a few months ago) but I agree with other commenters it's better than nothing and will almost surely improve the rates of testing/precaution around travel.
When I got the PCR COVID test administered when I had a suspected case, I was required to fill out a form stating my name, DOB, email, phone, physical address, full social security number, and student ID (I'm a college student). Since these are all attributes bound to identity, I'm sure it's not too difficult to make a database of test results.
...Just from the thought of it, forcing other countries to store your private info would be a terrible idea considering they probably could care less about it being stolen.
But, you are entirely missing the point. The U.S. cannot mandate that other countries maintain a database with U.S. citizens personal info, even if your idea didn't have massive gaping holes in it regarding security. It is simply impossible.
Forgeries of the international yellow fever vaccine certificate happen regularly. (For example, backpackers to Africa from Eastern European countries where the yellow fever vaccine was perennially unavailable at our local clinics printed out their own copy on yellow paper and put a fake stamp on it.) Nevertheless, the yellow-fever certificate requirement is believed to work well enough regardless. With COVID, too, one could argue that something is better than nothing.
I mean the number of people who are willing to commit forgery and lie to border patrol is probably pretty small. This is a huge step in the right direction that will prevent loads of air transmission. We don't really have time to wait years for a "fully baked" solution, and this is a solid compromise.
It doesn't need any of that to be nearly entirely effective. The vast majority of people traveling into the country are not going to attempt to falsify documents.
Don't leave during a pandemic then? When healthcare resources are stretched thin all around the world who is going to be able to take care of a sick foreigner or get them back to their country without endangering others?
If the world had enough N95 masks and everyone wore them this would be over, but instead we are wearing bandanas and pulling t- shirts up over our noses.
When you are vaccinated it is over for you. When everyone who wants to be vaccinated is vaccinated then it should be over for everyone. I would say the vaccine currently exists but is not widely available. I know vulnerable people with a lot of living left to do that can't wait to get out of the house.
It will be everyone's responsibility to ensure unnecessary restrictions are lifted.
Surprising it took so long. I wonder if you are going to get some sort of certificate that proves you have been vaccinated for COVID once they roll out to everyone.
Most of the countries that have sane case rates and many that are doing terribly with respect to case rate already require this. Some such as the Netherlands added it relatively recently for transit passengers as well, although most only require it for arrival passengers.
> U.S. officials do not plan to drop restrictions that were adopted starting in March that ban most non-U.S. citizens who have been in most of Europe, the United Kingdom and Brazil as soon as possible, the sources said.
Does anyone know if the EU travel ban is going to get lifted anytime this year (with the Biden administration)?
I’d sure hope it would be this year. Keep in mind we should have the ability to vaccinate every American adult by the late spring so the pandemic should be reduced to very low levels.
I'm all for this, but I'm somewhat surprised that this isn't being railed as "xenophobic"... wonder why we've suddenly had a change in heart on these topics?
It Seems like a good idea but I worry about the slippery slope effect.
Can they require this for flu? How will they handle false positives? What about something like HIV? What if you need to get home for medical treatment or a family emergency?
The slippery slope argument is generally regarded as a logical fallacy because the argument can be applied to anything. You should at least offer an explanation of why believe the slippery slope is a risk in this case. What interest would the U.S. have in requiring Flu or HIV tests for travel? The reasons for requiring a covid test are obvious unless you're a person that believes covid is equivalent to the flu.
> The slippery slope argument is generally regarded as a logical fallacy because the argument can be applied to anything.
Can you expand on this? I've seen the claim several times, but given the fact that (in general, not referring to covid) it is possible to point to historical examples of how things progress from A->B->C, and then you can identify a sequence of A->B currently, it becomes almost silly not to conclude the goal is C. So why is demonstrating history repeating itself a fallacy?
Granted I've placed a number of conditions there. Maybe that's what you mean. I'm just curious what the general argument is.
> What interest would the U.S. have in requiring Flu or HIV tests for travel?
Humans unfortunately have a bias for "doing something" rather than nothing, even if the two actions are equivalent in consequence (which favors doing nothing - less energy).
Scream loud enough and we'll create problems where there weren't any. I mean that's basically what network news does all day every day. Then we'll respond to those problems, and create more problems. Etc. "It worked for covid, why aren't we doing it for the flu?" Even if the argument isn't valid, it sounds good, and politicians like things that sound good even if they don't do anything, creating problems and great expense for people for little to no actual gain.
HIV/AIDS is definitely frequently considered a pandemic, and at least a global epidemic. In any case the obvious difference is that it isn't as contagious.
This will now place a strain on the testing facilities of small countries (islands) that are a popular destination of American tourists.
In Jamaica, every lab that has been approved to conduct the PCR test has been overwhelmed by a flood a Canadian tourists who now need a negative PCR test result to return home. Mind you, smaller countries have been having an uphill battle with procuring the reagents needed for the PCR tests because countries like the US is grabbing up everything COVID related, and not using them.
Had the US implemented these measures 9 months ago, the entire world would have looking at the tail-end of this pandemic, instead of waiting for the US to catchup with what every other country considers as a best practice.
Every other country? Have you looked at the recent COVID-19 case and death rates in much of western Europe? Many of those countries, one of which I live in (which still doesn't require testing arrival passengers), are still changing their policies on incoming travelers with respect to quarantining and testing. There isn't some global consensus that the US is blind to.
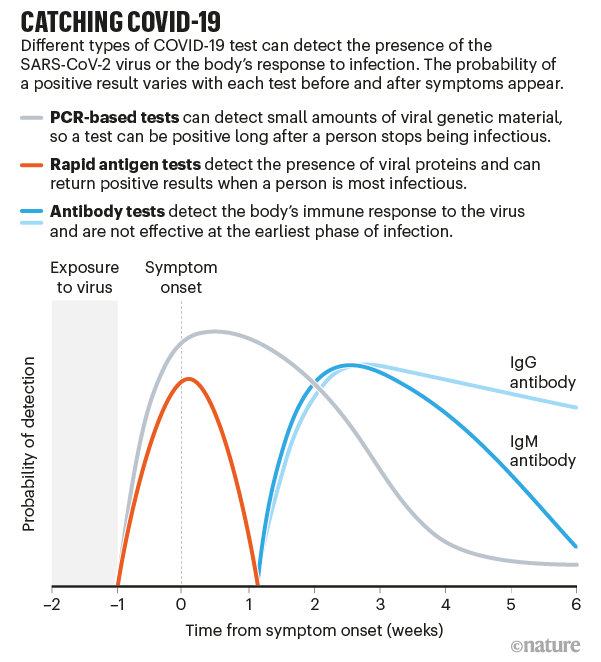{kind=link}
As it happens, I currently have COVID. When I first noticed I was getting sick, I was scheduled to fly in the near future, so I got a rapid COVID test that delivers results in 15 minutes.
It was negative. I got another one, and it was negative too. I had thus intended to go ahead with the trip under the assumption I had a minor cold.
Later, a few days before I was to fly, I lost all smell and taste. Now I didn’t know what to think. I wasn’t particularly congested, and the loss of smell was total. I’d never experienced this before. Could both tests have been false negatives?
I delayed the flight (free of charge luckily, so no big deal) and got a test that had to be sent to a lab for analysis. A week later, the positive test result came back.
Take from this what you will. I'm not a scientist or a doctor and frankly there's nothing remotely intelligent I can say about the various tests out there for COVID. But if the rapid tests are as unreliable in general as they were for me, it’s sort of no wonder COVID is spreading like wildfire. I was very, very close to boarding a plane with an active case of COVID, and I would have if I hadn’t acted out of an abundance of caution.